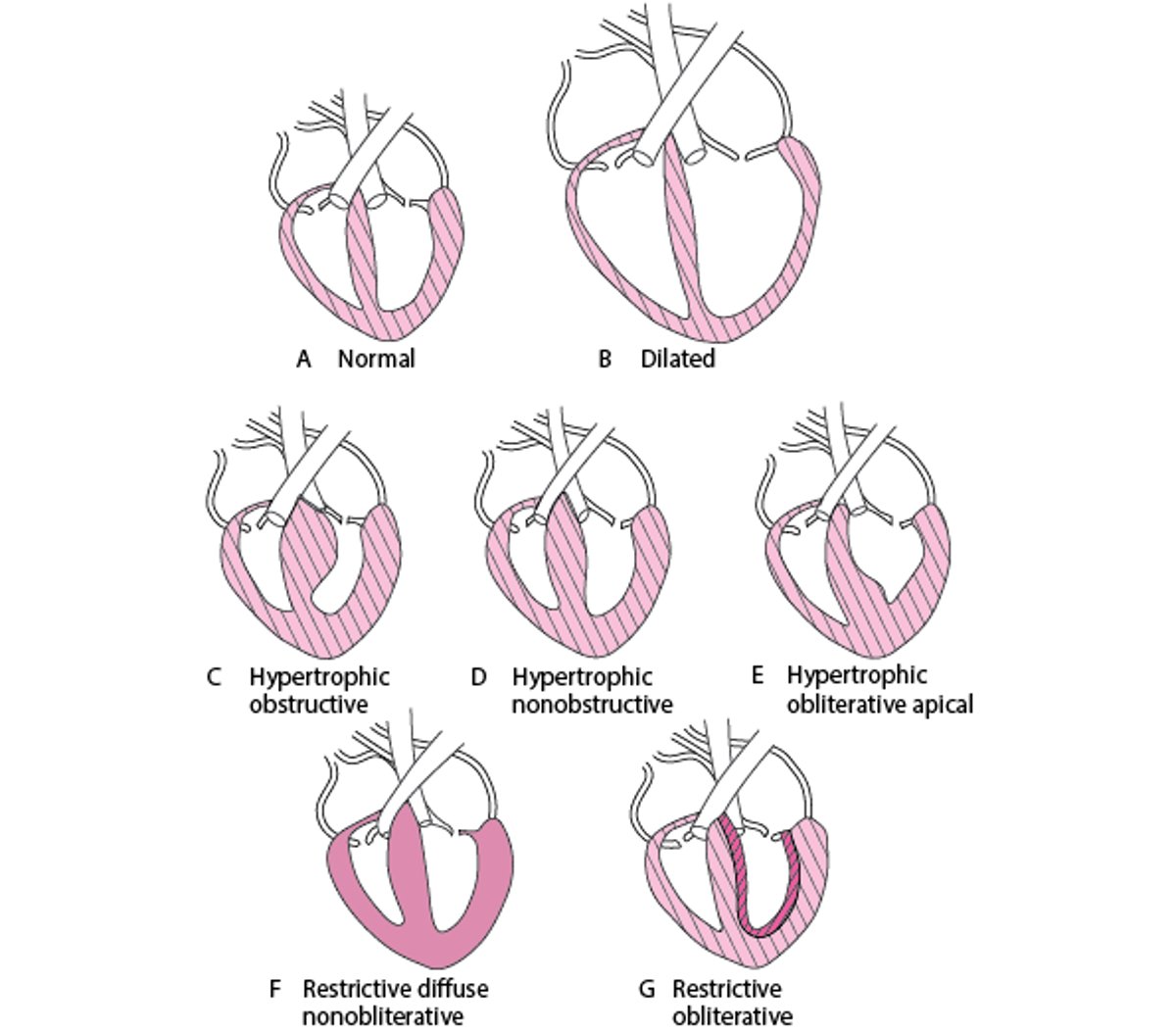
A cardiomyopathy is a primary disorder of the heart muscle. It is distinct from structural cardiac disorders such as coronary artery disease, valvular disorders, and congenital heart disorders. Cardiomyopathies are divided into 3 main types based on the pathologic features (see figure Forms of Cardiomyopathy):
The term ischemic cardiomyopathy refers to the dilated, poorly contracting myocardium that can occur in patients with severe coronary artery disease (with or without areas of infarction). It is not classically considered to be in the above-listed categories because it does not describe a primary myocardial disorder.
Manifestations of cardiomyopathies are usually those of heart failure and vary depending on whether there is systolic dysfunction, diastolic dysfunction, or both. Some cardiomyopathies may also cause chest pain, syncope, arrhythmias, or sudden death.
Evaluation typically includes family history, blood tests, ECG, chest x-ray, echocardiography, and cardiac MRI. Some patients require endomyocardial biopsy. Other tests are done as needed to determine the cause. Treatment depends on the specific type and cause of cardiomyopathy (see table Diagnosis and Treatment of Cardiomyopathies).
Forms of Cardiomyopathy