


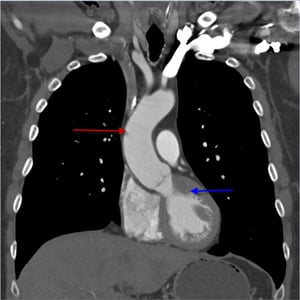
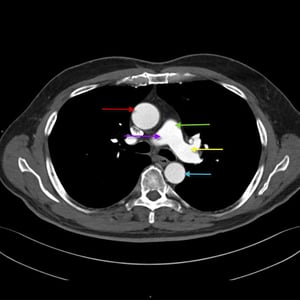
Aneurysms are abnormal dilations of arteries caused by weakening of the arterial wall. Common causes include hypertension, atherosclerosis, infection, trauma, systemic rheumatic diseases, and connective tissue disorders (eg, Marfan syndrome, Ehlers-Danlos syndrome). Aneurysms are usually asymptomatic but can cause pain and lead to ischemia, thromboembolism, spontaneous dissection, and rupture, which may be fatal. Diagnosis is by imaging tests (eg, ultrasonography, CT angiography, magnetic resonance angiography, aortography). Unruptured aneurysms may be treated with medical management or repaired, depending on symptoms and the size and location of the aneurysm. Medical management includes risk factor modification (eg, strict blood pressure control) plus scheduled surveillance imaging. Repair can be done with either an open surgical or endovascular approach. Treatment of ruptured aneurysms is immediate repair.
The aorta originates at the left ventricle above the aortic valve, travels upward (ascending thoracic aorta) to the first branch of the aorta (brachiocephalic or innominate artery), arches up and behind the heart (aortic arch), then turns downward distal to the left subclavian artery (descending aorta) through the thorax (thoracic aorta) and abdomen (abdominal aorta). The abdominal aorta ends by dividing into the right and left common iliac arteries.
© 2017 Elliot K. Fishman, MD.

© 2017 Elliot K. Fishman, MD.
© 2017 Elliot K. Fishman, MD.

© 2017 Elliot K. Fishman, MD.


© 2017 Elliot K. Fishman, MD.


© 2017 Elliot K. Fishman, MD.


© 2017 Elliot K. Fishman, MD.

© 2017 Elliot K. Fishman, MD.
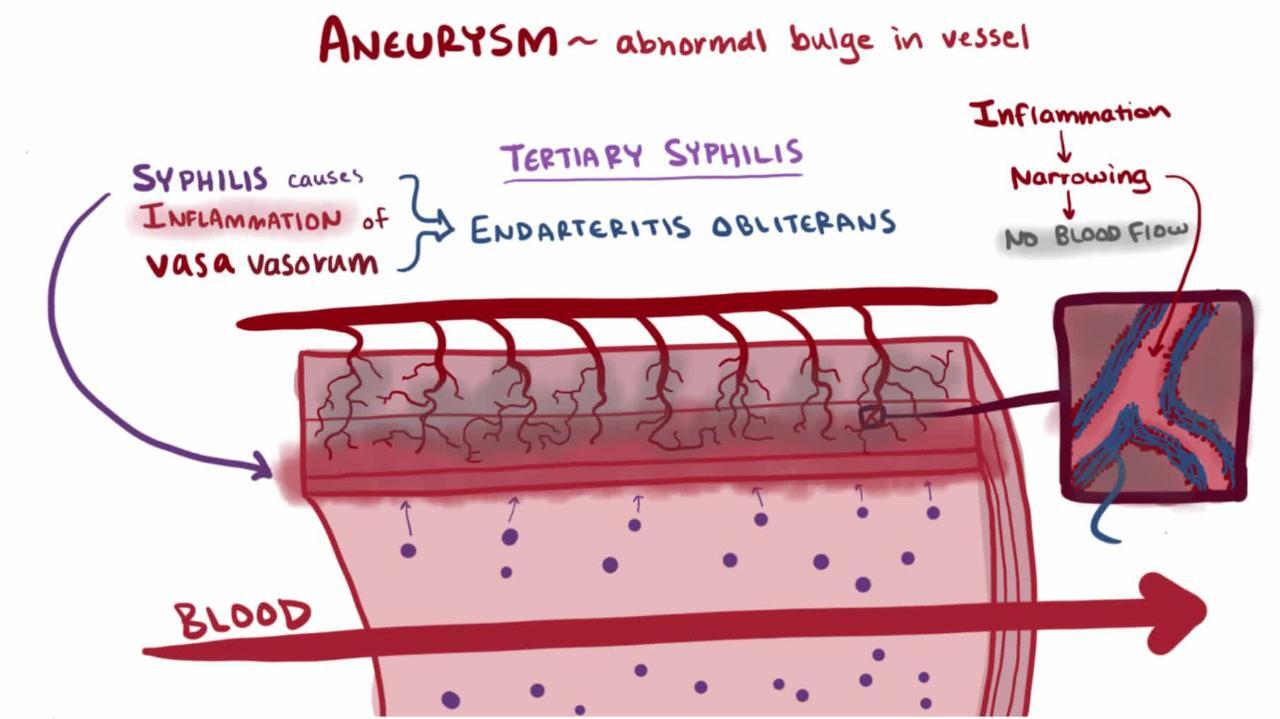
The wall of the aorta is composed of three layers:
Intima: A thin layer lined with endothelium
Media: A thick layer of elastic fibers arranged in spiral formation
Adventitia: A thin fibrous layer containing the nutrients for the media
Aneurysms are abnormal dilations of arteries defined as a ≥ 50% increase in arterial diameter compared with normal segments. They are caused by weakening of the arterial wall, specifically, the media. True aneurysms involve all 3 layers of the artery (intima, media, and adventitia). Aneurysmal disease is not usually a focal problem (eg, often resulting from multiple factors) and can extend along the aorta with time.
A pseudoaneurysm (false aneurysm) is a communication between the arterial lumen and overlying connective tissue resulting from arterial rupture; a blood-filled cavity forms outside the vessel wall and seals the leak as it thromboses.
Aneurysms are classified as
Fusiform: Circumferential widening of the artery
Saccular: Localized, typically asymmetric, outpouchings of the artery wall
Layered (laminated) thrombus may line the walls of either type as the result of alterations in flow within the aneurysmal segment.
Aneurysms may occur in any artery. The most common and significant are
Aneurysms of the major aortic branches (subclavian and splanchnic arteries) are much less common. Aneurysms of peripheral arteries and the cerebrovascular system (causing stroke) are discussed elsewhere.






