It is important to understand the anatomy of the eye prior to doing an examination.
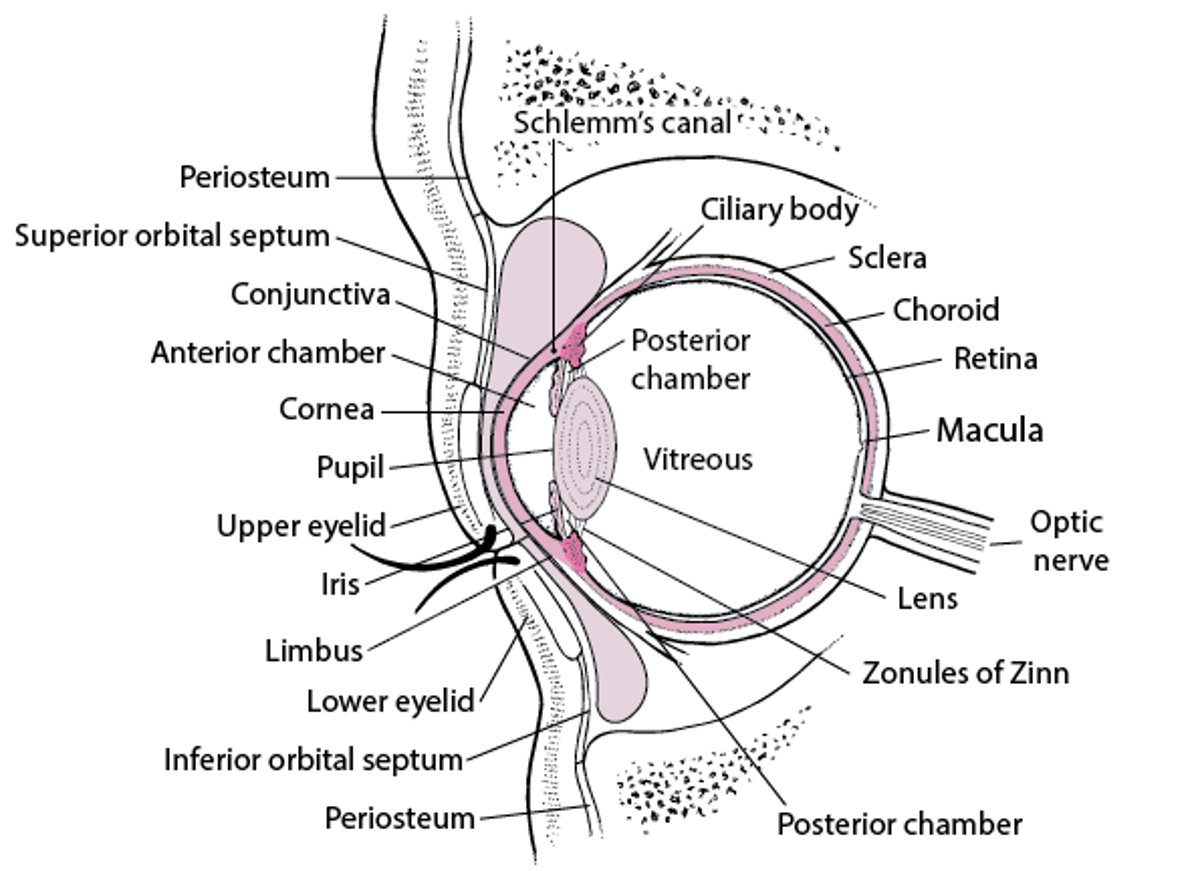
Cross-section of the eye
The zonules of Zinn keep the lens suspended, and the muscles of the ciliary body focus the lens. The ciliary body also secretes aqueous humor, which fills the anterior and posterior chambers, passes through the pupil into the anterior chamber, and drains primarily via Schlemm’s canal. The iris regulates the amount of light entering the eye by adjusting the size of its central opening, the pupil. Visual images are focused on the retina. The fovea centralis is the area of sharpest visual acuity. The conjunctiva covers the eyeball and lines the upper and lower eyelids; it ends at the limbus. The cornea is covered with epithelium that is more sensitive than and differs from the conjunctival epithelium. |