Voluntary movement requires complex interaction of the corticospinal (pyramidal) tracts, basal ganglia, and cerebellum (the center for motor coordination) to ensure smooth, purposeful movement without extraneous muscular contractions.
The pyramidal tracts pass through the medullary pyramids to connect the cerebral cortex to lower motor centers of the brain stem and spinal cord.
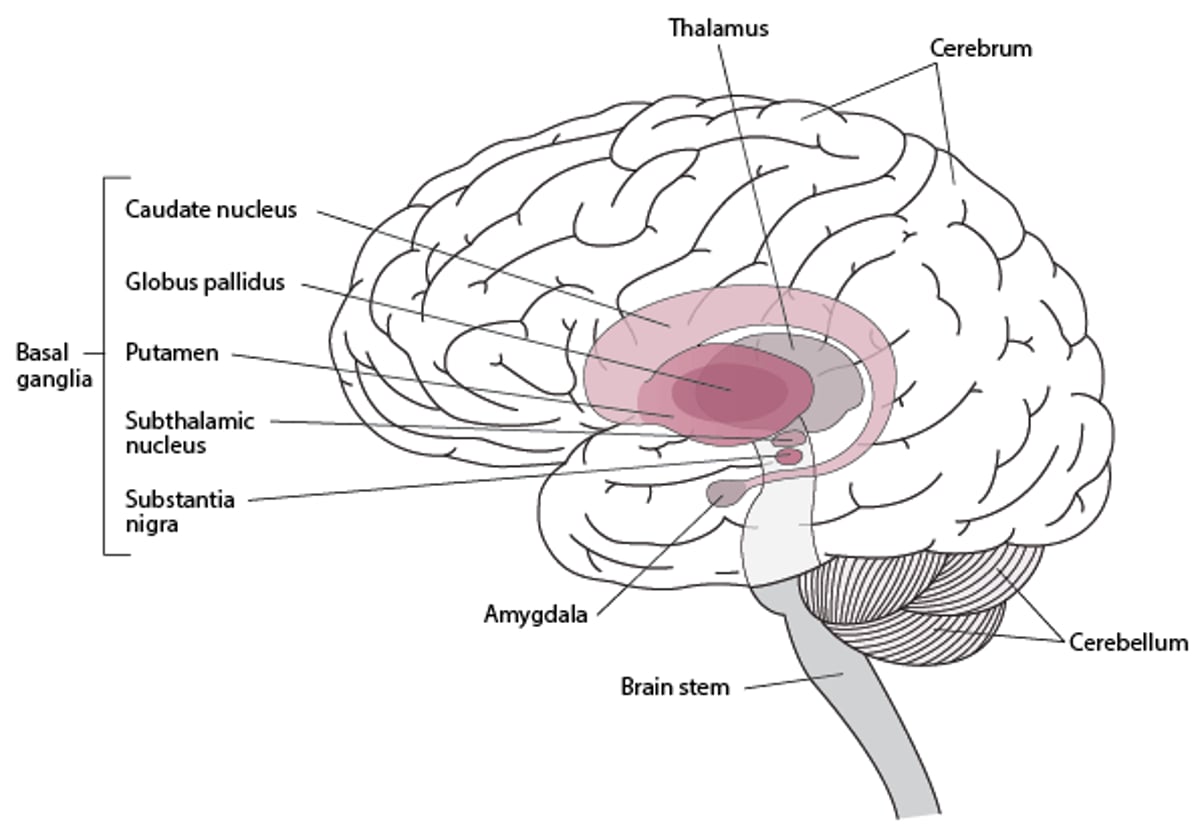
The basal ganglia (caudate nucleus, putamen, globus pallidus, subthalamic nucleus, and substantia nigra) form the extrapyramidal system. They are located deep in the forebrain and rostral midbrain. The basal ganglia direct their output mainly through the thalamus to the cerebral cortex (see figure Basal Ganglia). Two main motor functions are integrated in the basal ganglia:
Operational learning (motor tasks)
Task selection (whether single, dual or multiple as when walking and speaking)
Most neural lesions that cause movement disorders occur in the extrapyramidal system; thus, movement disorders are sometimes called extrapyramidal disorders.

Basal Ganglia

Classification of Movement and Cerebellar Disorders
Movement disorders are commonly classified as those with
Decreased or slow movement (hypokinetic disorders)
Increased movement (hyperkinetic disorders)
The classic and most common hypokinetic disorder is
Hyperkinetic disorders refer to
Chorea (including hemiballismus [rapid chorea] and athetosis [slow chorea])
Stereotypies
Akathisia
However, this classification does not account for overlap between categories (eg, tremors that occur in Parkinson disease).
Cerebellar disorders are sometimes considered hyperkinetic disorders often accompanied by axial, gait, and appendicular ataxia with or without central nystagmus, ocular saccadic dysmetria, and pursuit dysfunction.
Hyperkinetic disorders
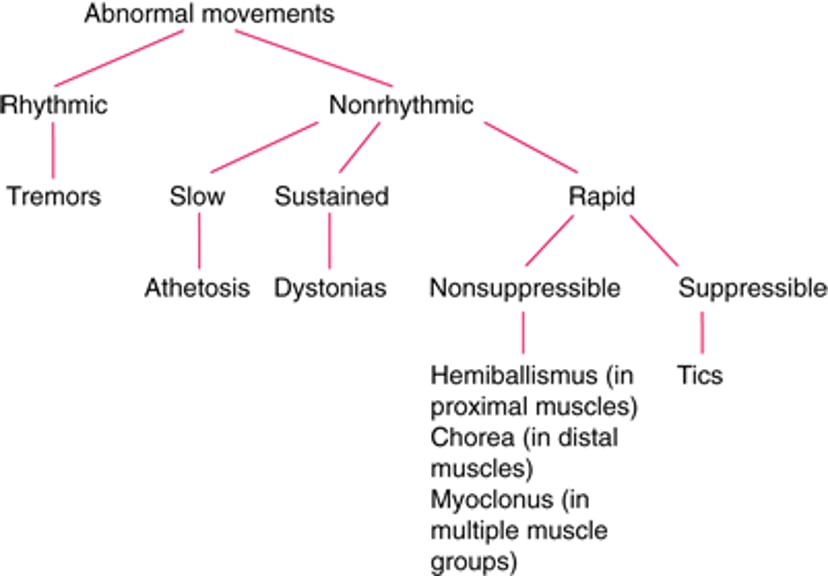
Hyperkinetic disorders (see figure Classification of Common Hyperkinetic Disorders and table Hyperkinetic Disorders) can be
Rhythmic
Nonrhythmic
Rhythmic disorders are primarily tremors—regular alternating or oscillatory movements, which can occur mainly at rest, while maintaining a position, and/or during attempted movement. However, in some cases, a tremor, though rhythmic, is irregular, as occurs when tremor is associated with dystonic disorders.
Nonrhythmic hyperkinetic disorders can be
Slow (eg, athetosis)
Sustained (eg, dystonias)
Rapid (eg, myoclonus, chorea, tics, hemiballismus)
Rapid nonrhythmic hyperkinetic disorders may be
Suppressible (eg, tics)
Nonsuppressible (eg, hemiballismus, chorea, myoclonus)
Athetosis and chorea may occur together as choreoathetosis. Chorea is the most characteristic movement disorder in Huntington disease.
Multiple motor and phonatory tics are the defining feature of Tourette syndrome.
Classification of Common Hyperkinetic Disorders