


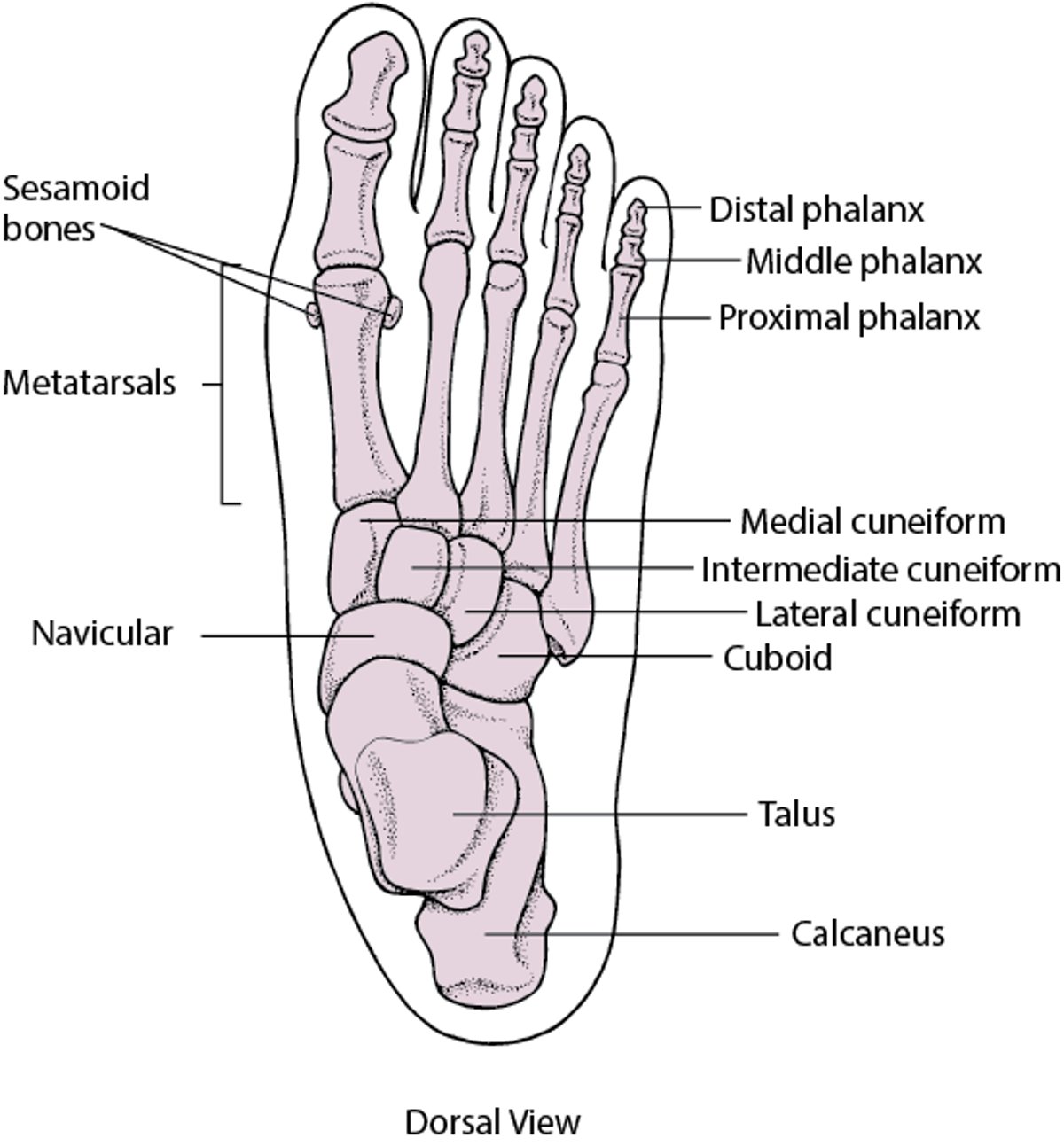
Most foot problems result from anatomic disorders or abnormal function of articular or extra-articular structures (see figure Bones of the Foot). Less commonly, foot problems reflect a systemic disorder (see table Foot Manifestations of Systemic Disorders).

In people with diabetes and/or peripheral arterial disease, careful examination of the feet, with evaluation of vascular sufficiency and neurologic integrity, should be done at least twice a year. People with these diseases should examine their own feet at least once a day.
The feet are also common sites for musculoskeletal pain, pressure and friction injuries, and infections by fungus, bacteria, and viruses.
See also table Common Foot and Ankle Disorders by Anatomic Site and table Disorders Associated With Heel Pain According to Location.
Bones of the Foot

Considerations for Using Corticosteroid Injections
Corticosteroid injections should be used judiciously to avoid adverse effects. Injectable corticosteroids should be reserved for inflammatory conditions such as gout and rheumatoid arthritis). Because the tarsus, ankle, retrocalcaneal space, and dorsum of the toes have little connective tissue between the skin and underlying bone, injection of insoluble corticosteroids into these structures may cause depigmentation, atrophy, or ulceration, especially in older patients with peripheral arterial disease.
Insoluble corticosteroids can be given deeply rather than superficially with greater safety (eg, in the heel pad, tarsal canal, or metatarsal interspaces). The foot should be immobilized for a few days after tendon sheaths are injected. Unusual resistance to injection suggests injection into a tendon. The use of ultrasound guidance can improve the accuracy of the injection and, depending on the location, may also improve efficacy (1). Repeated injection into a tendon should be avoided because the tendon may weaken (partially tear), predisposing to subsequent rupture.
Reference
1. Daniels EW, Cole D, Jacobs B, Phillips SF: Existing evidence on ultrasound-guided injections in sports medicine. Orthop J Sports Med 6(2):2325967118756576, 2018. Published 2018 Feb 22. doi:10.1177/2325967118756576






