


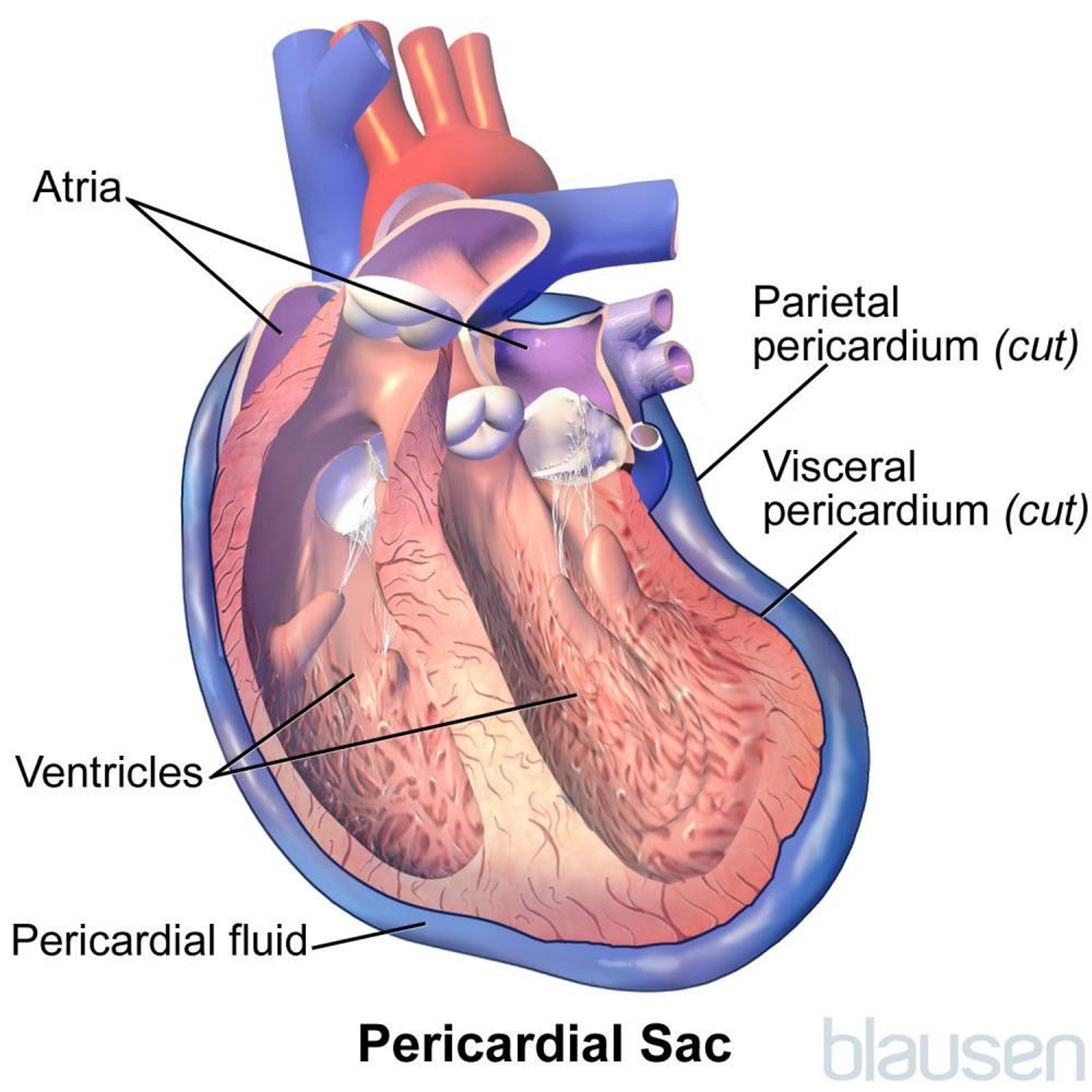
Acute pericarditis is inflammation of the pericardium (the flexible two-layered sac that envelops the heart) that begins suddenly, is often painful, and causes fluid and blood components such as fibrin, red blood cells, and white blood cells to enter the pericardial space.
Certain infections and other conditions that inflame the pericardium cause pericarditis.
Fever and chest pain, which is sharp and varies with position and movement and occasionally may feel like a heart attack, are common symptoms.
Doctors base the diagnosis on symptoms and occasionally by hearing a tell-tale sound when listening to the heartbeat with a stethoscope.
People are often hospitalized and given drugs to reduce pain and inflammation.
(See also Overview of Pericardial Disease and Chronic Pericarditis.)
Sometimes the inflammation can cause excess fluid to enter the pericardial space (pericardial effusion). Sometimes, when pericarditis is due to an injury, cancer, or heart surgery, the fluid is blood.

Causes of Acute Pericarditis
Causes of acute pericarditis include
Infection (viral, bacterial, parasitic, or fungal and, in people with AIDS, tuberculosis, or aspergillosis)
Heart surgery (postpericardiotomy syndrome)
Systemic lupus erythematosus (lupus)
Chest injury
Cancer (such as leukemia, breast cancer, or lung cancer, or, in people with AIDS, Kaposi sarcoma)
Radiation therapy
Unknown (idiopathic or nonspecific pericarditis)
In people who have AIDS, a number of infections, including tuberculosis and aspergillosis, may result in pericarditis. Pericarditis due to tuberculosis (tuberculous pericarditis) accounts for less than 5% of cases of acute pericarditis in the United States but accounts for the majority of cases in some areas of India and Africa. SARS-CoV-2 infection infrequently causes pericarditis.
After a heart attack, acute pericarditis develops during the first day or two in 10 to 15% of people and after about 10 days to 2 months in 1 to 3% (subacute pericarditis). Subacute pericarditis is caused by the same disorders that cause acute pericarditis.
Symptoms of Acute Pericarditis
Usually acute pericarditis causes sharp chest pain, which often extends to the left shoulder and sometimes down the left arm. The pain may be similar to that of a heart attack, except that it tends to be made worse by lying down, swallowing food, coughing, or even deep breathing. The accumulating fluid or blood in the pericardial space puts pressure on the heart, interfering with its ability to pump blood. If the pressure is too high, cardiac tamponade—a potentially fatal condition—may occur. Sometimes acute pericarditis does not cause any symptoms.
Pericarditis due to tuberculosis begins insidiously, sometimes without obvious symptoms of infection. It may cause fever and symptoms of heart failure, such as weakness, fatigue, and difficulty breathing. Cardiac tamponade may occur.
Acute pericarditis due to a viral infection is usually painful but short-lived and has no lasting effects.
When acute pericarditis develops in the first day or two after a heart attack, symptoms of pericarditis are seldom noticed because symptoms of the heart attack are the main concern.
Pericarditis that develops about 10 days to 2 months after a heart attack is usually accompanied by postmyocardial infarction syndrome (Dressler syndrome), which includes fever, pericardial effusion (extra fluid in the pericardial space), pleuritic pain (pain due to inflammation of the pleura, which are the membranes covering the lungs), pleural effusion (fluid between the two layers of the pleura), and joint pain.
Symptoms of acute pericarditis often go away on their own but come back in up to 30% of people.
In 15 to 25 percent of people with idiopathic pericarditis, symptoms recur on and off for months or years (called recurrent pericarditis).
Diagnosis of Acute Pericarditis
Electrocardiography
Chest x-ray
Echocardiography
Tests to identify the cause
Doctors can usually diagnose acute pericarditis based on the person's description of the pain and the sounds heard by listening through a stethoscope placed on the person's chest. Pericarditis can cause a crunching sound similar to the creaking of a leather shoe or a scratchy sound similar to the rustling of dry leaves (pericardial rub). Doctors can often diagnose pericarditis a few hours to a few days after a heart attack based on hearing these sounds.
Usually, doctors also do electrocardiography (ECG), which often shows abnormalities caused by the pericarditis. Then doctors look for signs of pericardial effusion by doing a chest x-ray and echocardiography (a procedure that uses ultrasound waves to produce an image of the heart).
Tests for the cause of pericarditis
Sometimes the cause of pericarditis is obvious, such as a recent heart attack. Other times the cause may not be clear.
Echocardiography may suggest the cause—for example, the image shown on the echocardiogram or chest x-ray may suggest cancer.
Blood tests can detect some of the other conditions that cause pericarditis—for example, leukemia, infections, rheumatic fever
If the cause of pericarditis remains unknown, doctors may withdraw a sample of the pericardial fluid and/or pericardial tissue using a needle inserted through the chest wall (pericardiocentesis). The fluid and tissue are sent to the laboratory for testing.
Prognosis of Acute Pericarditis
The prognosis for people who have pericarditis depends on the cause. When pericarditis is caused by a virus or when the cause is not apparent, recovery usually takes 1 to 3 weeks. Complications or recurrences can slow recovery. People with cancer that has invaded the pericardium rarely survive beyond 12 to 18 months.
Treatment of Acute Pericarditis
Treatment of the underlying disorder, such as cancer
Infrequently, surgical treatment such as pericardiotomy
nonsteroidal anti-inflammatory drugs [NSAIDs], myopericarditis [pericarditis involving the heart muscle as well as the pericardium] and moderate or large pericardial effusions). The person is monitored for complications, particularly cardiac tamponade.
Anti-inflammatory drugs
Treating the underlying disorder
Further treatment of acute pericarditis varies, depending on the cause. For people who have kidney failure, increasing the frequency of dialysis usually results in improvement.
Drugs that may cause pericarditis are stopped whenever possible.
People who have cancer may respond to chemotherapy or radiation therapy.
If a bacterial infection is the cause, treatment consists of antibiotics and surgical drainage of pus from the pericardium.
Surgical treatment
Fluid may be drained from the pericardium by inserting a thin catheter into the pericardial space (pericardiocentesis).
Sometimes a balloon-tipped catheter is inserted through the skin. The balloon is then inflated to create a hole (window) in the pericardium. This procedure, called percutaneous balloon pericardiotomy, is usually done as an alternative to surgery when effusions are due to cancer or recur.
Alternatively, a small incision is made below the breast bone, and a piece of the pericardium is removed. Then a tube is inserted into the pericardial space. This procedure, called a subxiphoid pericardiotomy, is often done when effusions are due to bacterial infections. Both procedures require a local anesthetic, can be done at the person's bedside, allow fluid to drain continuously, and are effective.






