


A spinal cord injury is damage to the bundle of cells and nerves that carry incoming and outgoing messages between the brain and the rest of the body.
Most spinal cord injuries result from motor vehicle crashes, falls, assaults, and sports injuries.
Symptoms, such as loss of sensation, loss of muscle strength, and loss of bowel, bladder, and sexual function, may be temporary or permanent.
Magnetic resonance imaging (to assess injury to soft tissue, spinal cord, or ligaments) and/or computed tomography (to assess injury to bone) is the best way to identify the injury.
Treatment involves immobilization of the spine, medications to relieve symptoms, sometimes surgery, and usually rehabilitation.
The spine consists of 24 back bones (vertebrae) plus the tailbone (sacrum). The vertebrae bear most of the body's weight and thus are under a lot of pressure. Disks of cartilage between vertebrae help cushion and protect the bones. The spine forms a protective canal of bone in which the spinal cord is encased.
The spinal cord is a long, fragile tubelike structure that begins at the end of the brain stem and continues down to the lower part of the spine. The spinal cord consists of nerves that carry incoming and outgoing messages between the brain and the rest of the body. (See also Spinal Cord.)

Spinal injuries may affect the bones of the spine, the spinal cord, or the roots of the spinal nerves (short branches of the spinal nerves), which pass through the spaces between the vertebrae. The bundle of nerve roots that extend downward from the end of the spinal cord (cauda equina) may also be injured. Injuries of the spinal cord cause nerve damage or dysfunction in one the following ways:
Jarring by a blunt injury (such as a fall or a collision)
Pressure (compression) by broken bones, swelling, or an accumulation of blood (hematoma)
Partial or complete tears (severing)
Because the spinal cord is surrounded and protected by the spine, injuries of the spine or its connective tissue (such as disks and ligaments—see figure A Herniated Disk) can also injure the spinal cord. Such injuries include the following:
Fractures
Complete separation (dislocation) of adjacent vertebrae
Partial misalignment (subluxation) of adjacent vertebrae
Loosened ligament attachments (composed of connective tissue) between adjacent vertebrae
Ligaments may be loosened so much that the vertebrae move freely. These injuries are considered unstable. When vertebrae move, they can compress the spinal cord or its blood supply and damage spinal nerve roots. An unstable injury to the spine may not damage the spinal cord immediately. For example, the injury may cause spasms of muscles supporting the spine that prevent the vertebrae from moving much. However, after hours or days, muscle spasms may subside, enabling the vertebrae to move freely, which can damage the spinal cord.
Almost all people with a spinal cord injury have an injury to the spine. However, sometimes children do not (see Spinal Cord Injury in Children).
The most common cause of spinal cord injuries is motor vehicle crashes, accounting for almost half of them. Other causes include falls, sports, work-related injuries, and violence (such as a knife or gunshot wound).
Among older people, falls are the most common cause. Older people are also at higher risk of serious spinal injuries because conditions such as osteoporosis and osteoarthritis (degenerative joint disease) are more common among older people.
Symptoms of Spinal Injuries
If the spine is injured, people usually feel pain in the affected part of the neck or back. The area over the injury may be tender to the touch, particularly if a fracture is present. If the spinal cord is injured, the nerves at and below the site of the injury malfunction, causing loss of muscle control and loss of sensation. However, children may have spinal cord injuries in which nerves malfunction only temporarily and briefly. They may have lightning-like pains that shoot down the arms or legs.
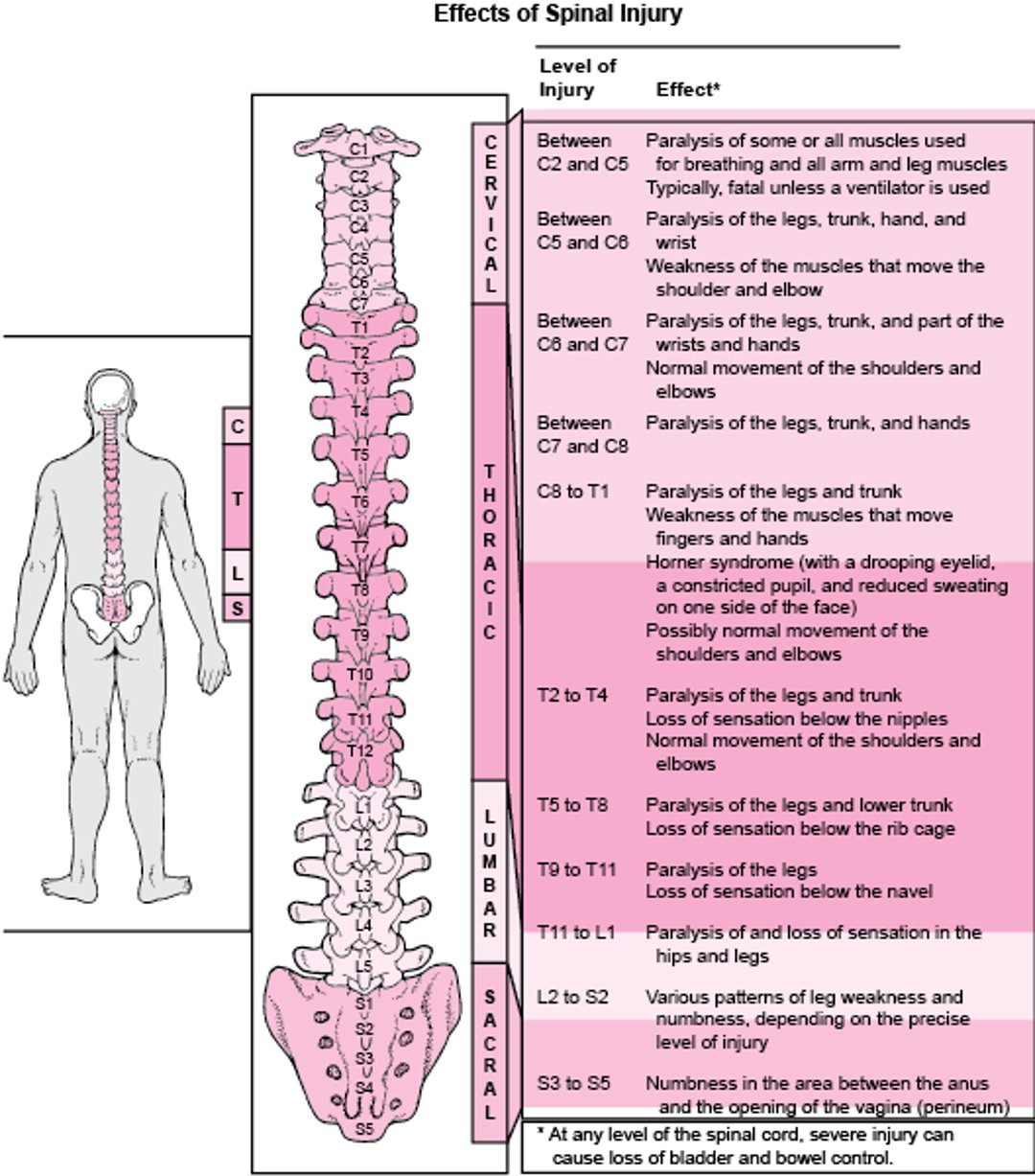
Exactly what and how much function is lost in the arms and legs depends on the location of the spinal cord injury. For example, if the spinal cord is injured in the neck, the person may lose movement and sensation in both the arms and the legs, whereas an injury farther down the spinal cord may result in dysfunction in the legs only. A person can lose control of the ability to urinate or have a bowel movement and lose sexual function regardless of the location of the spinal cord injury.
When nerve damage occurs, loss of muscle control or sensation may be temporary or permanent, partial or total, depending on the severity of the injury. An injury that severs the spinal cord or destroys nerve pathways in the spinal cord causes permanent paralysis, but a blunt injury that jars the spinal cord may cause temporary weakness, which can last days, weeks, or months. Sometimes swelling causes symptoms that suggest an injury more severe than it is, but the symptoms usually lessen as the swelling subsides.
Partial loss of muscle control results in muscle weakness. Paralysis usually refers to complete loss. When muscles are paralyzed, they often go limp (flaccid), losing their tone. Muscle reflexes that doctors check using a reflex hammer are weak or absent. But when the spinal cord is injured, paralysis may progress weeks later to involuntary, prolonged muscle spasms (called spastic paralysis). In this case, muscle reflexes are stronger than normal.
Where Is the Spinal Cord Damaged?

Complications of spinal cord injury
For people who are weak or paralyzed, movement is limited or impossible. Consequently, they are at risk of developing blood clots, pressure sores, permanently shortened muscles (contractures), urinary tract infections, and pneumonia.
Diagnosis of Spinal Injuries
Imaging
People who have symptoms of spine injury (such as significant pain in the bones of the neck or back) and children who have even brief symptoms of possible nerve damage or pains that shoot down the arms or legs need to be evaluated in an emergency department.
Injuries to the spine (affecting bones) and spinal cord are diagnosed by imaging tests.
X-rays: After an injury, an x-ray is often done. X-rays can be done immediately, usually while the person is still in an emergency department. X-rays can show injuries of the bones in the spine but do not show injuries of the spinal cord.
Computed tomography (CT): Whether or not x-rays are done, CT is done after a spinal injury. CT is the most accurate test for injuries of the spine and can show most bony injuries.
Magnetic resonance imaging (MRI): MRI is the best test for injuries of the spinal cord and the ligaments of the spine. However, CT is generally done before MRI is done because MRI is less readily available than CT and does not show injuries to bone in as much detail as CT.
Although MRI is best suited for assessing the spinal cord and ligaments of the spine, occasionally MRI is not possible due to implanted devices such as pacemakers. In these cases, CT myelography may be done. CT myelography is a CT scan done after doctors inject a radiopaque dye into the space around the spinal cord. CT myelography can show displaced structures that impinge on the spinal cord.
Treatment of Spinal Injuries
Immobilization
Surgery to stabilize the spine when appropriate
Rehabilitation
People who may have a spinal cord injury should not be moved except by emergency personnel. The initial goals are to make sure people can breathe and to prevent further damage. Thus, emergency personnel take great care to keep the neck immobile when moving a person with a possible spinal cord injury. Usually, the person is strapped to a firm board and carefully padded to prevent movement. A rigid collar may be used to keep the neck from moving. When the spine is severely damaged, the vertebrae may no longer be held in place or may be broken, making the spine unstable. Thus, even slight movement of the injured person can cause the spine to shift, putting pressure on the spinal cord. Pressure on the cord increases the risk of permanent paralysis.


Surgery is needed to remove blood and bone fragments if they have accumulated and are pressing on the spinal cord. If the spine is unstable, the person is immobilized until the bone and other tissues have had time to heal. Sometimes a surgeon implants steel rods to stabilize the spine so that it cannot move and cause additional injury. The best time for surgery is debated. Spinal surgery may be done by neurosurgeons or orthopedic surgeons.
Medications may be useful.
Good nursing care can help prevent complications due to bed rest, such as pressure sores, urinary tract infections, blood clots in the legs, and pneumonia.
Experimental treatments to stimulate growth of spinal nerves are being studied. For example, a certain type of white blood cell (macrophage) can be extracted from the blood, then injected back into the injured person. The injected macrophages help speed the removal of waste products generated by the body’s reaction to the injury and secrete substances that may help the nerves regenerate. Experimental medications can be injected into the space around the spinal cord (epidurally) or taken by mouth. Using stem cells (unspecialized cells from which other, more specialized cells can be derived) is another possibility, but this treatment requires much more study. Researchers are also investigating using various surgical techniques to relieve pressure that builds up in the sac around the spinal cord after injury.
Rehabilitation, including physical and occupational therapy, can help people recover more quickly or more completely. People usually need emotional support, and often counseling and antidepressants, because depression usually develops when injury results in disability.
Prognosis for Spinal Injuries
Recovery is more likely if paralysis is partial and if movement or sensation starts to return during the first week after the injury. If function is not regained within 6 months, loss is likely to be permanent. However, several studies have shown that some recovery is possible up to one year after injury.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
United Spinal Association: This organization empowers people with spinal cord injuries to live full lives by providing information on emergency preparedness, hosting support groups for those with spinal cord injuries and their loved ones, and working to strengthen the Americans With Disabilities Act.






