


Smoking, chronic pancreatitis, obesity, and exposure to certain chemicals are risk factors for pancreatic cancer.
Abdominal pain, weight loss, jaundice, and vomiting are some typical symptoms.
Computed tomography or magnetic resonance imaging followed by endoscopic ultrasonography and biopsy are diagnostic techniques.
Treatment is a combination of surgery and chemotherapy.
Pancreatic cancer is usually fatal.
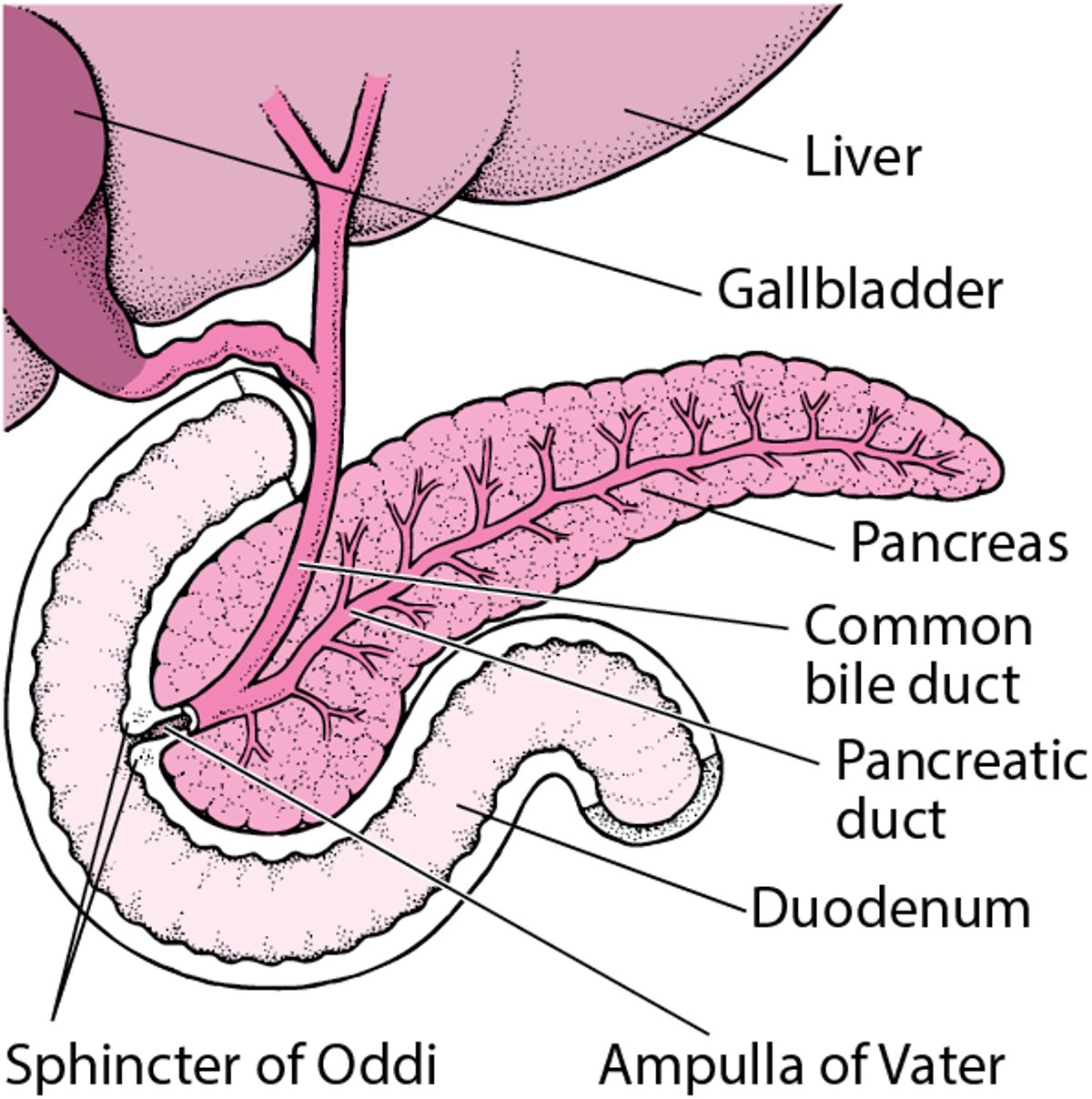
The pancreas is an organ located in the upper part of the abdomen. It produces digestive juices that are secreted into the digestive tract. The pancreas also produces insulin, which helps control blood sugar.
Most cancerous (malignant) tumors of the pancreas are adenocarcinomas. Adenocarcinomas usually originate in the cells lining the pancreatic duct. Most adenocarcinomas occur in the head of the pancreas, the part nearest the first segment of the small intestine (duodenum).
Locating the Pancreas

Adenocarcinoma of the pancreas has become increasingly common in the United States, occurring in an estimated 64,050 people each year and causing about 50,550 deaths each year. Adenocarcinoma usually does not develop before age 50. The average age at diagnosis is 55. These tumors are nearly twice as common among men.
Risk factors for pancreatic cancer include
Smoking
Exposure to certain chemicals (for example, asbestos, benzene, and chlorinated hydrocarbons)
Adenocarcinoma of the pancreas is more common among smokers than nonsmokers. People with chronic pancreatitis are at greater risk as well. People who have relatives with the disease may be at increased risk.
Alcohol and caffeine consumption do not seem to be risk factors.
Rare types of pancreatic cancer
Cystadenocarcinoma of the pancreas is a rare type of pancreatic cancer that develops from a fluid-filled noncancerous (benign) tumor called a cystadenoma. It often causes upper abdominal pain and may grow large enough for a doctor to feel it through the abdominal wall.
The diagnosis is usually made by a special type of computed tomography (CT) scan or magnetic resonance imaging (MRI) of the abdomen.
Only 20% of people with cystadenocarcinoma have tumors that have metastasized (spread) by the time surgery is done. Therefore, cystadenocarcinoma has a much better prognosis than adenocarcinoma. If the cancer has not spread and the whole pancreas is removed surgically, the person has a 65% chance of surviving for at least 5 years.
Intraductal papillary-mucinous neoplasm is a rare type of pancreatic tumor characterized by enlargement (dilation) of the main pancreatic duct, mucus overproduction, recurring episodes of pancreatitis, and occasional pain. These tumors can be cancerous or noncancerous.
The diagnosis of intraductal papillary-mucinous neoplasm is made by CT or MRI, and sometimes by endoscopic ultrasound (which shows the lining of the digestive tract more clearly because the probe is placed on the tip of the endoscope), with biopsy and analysis of the cyst fluid.
Treatment is usually surgery. With surgery, people with noncancerous intraductal papillary-mucinous tumors have a greater than 95% chance of surviving for 5 years. People with cancerous intraductal papillary-mucinous tumors have a 50 to 75% chance of surviving 5 years.
Symptoms of Pancreatic Cancer
In the early stages, pancreatic cancer typically causes no symptoms until the tumor has grown large. Thus, at the time of diagnosis, the tumor has already spread (metastasized) beyond the pancreas in 90% of cases.
Eventually, most people develop severe upper abdominal pain, which may also be felt in the middle of the back. The pain may be relieved by bending forward or assuming the fetal position.
Weight loss is common.
Complications of pancreatic cancer
Adenocarcinomas in the head of the pancreas can interfere with the drainage of bile (the digestive fluid produced by the liver) into the small intestine (see Gallbladder and Biliary Tract). Therefore, jaundice (a yellowish discoloration of the skin and the whites of the eyes) caused by obstruction of bile flow is typically an early symptom. The jaundice is accompanied by itchiness all over the body resulting from the deposit of bile salt crystals under the skin. Vomiting may result from instances when cancer in the head of the pancreas obstructs the flow of stomach contents into the small intestine (gastric outlet obstruction) or obstructs the small intestine itself.
Adenocarcinomas in the body or tail of the pancreas may obstruct the vein draining the spleen (the organ that produces, monitors, stores, and destroys blood cells), resulting in enlargement of the spleen (splenomegaly). Obstruction can also cause the veins to become swollen and twisted (varicose) around the esophagus (esophageal varices) and stomach. Severe bleeding may result, particularly from the esophagus, if these varicose veins rupture.
Certain cells in the pancreas produce insulin, a hormone that is essential to control blood sugar levels. Lack of insulin causes diabetes. Thus, because pancreatic cancer cells replace normal pancreatic cells, diabetes develops in up to half of people with pancreatic cancer, which leads to symptoms of high blood sugar, such as frequently urinating large volumes and excessive thirst.
Pancreatic cancer can also interfere with production of digestive enzymes by the pancreas, resulting in problems breaking down food and absorbing nutrients (malabsorption). This malabsorption causes bloating and gas and a watery, greasy, and/or foul-smelling diarrhea, leading to weight loss and vitamin deficiencies.
Diagnosis of Pancreatic Cancer
Computed tomography (CT) or magnetic resonance imaging/magnetic resonance cholangiopancreatography (MRI/MRCP) followed by endoscopic ultrasonography with biopsy
Early diagnosis of tumors in the body or tail of the pancreas is difficult because symptoms occur late and physical examination and blood test results are often normal. When adenocarcinoma of the pancreas is suspected, the preferred tests are CT or a specialized type of MRI called MRCP (see Magnetic Resonance Imaging). These imaging tests are usually followed by endoscopic ultrasonography (a tiny ultrasound probe on the tip of an endoscope is passed through the mouth into the stomach and the first segment of the small intestine). A tissue sample (biopsy) can be taken through the endoscope during the procedure.
To confirm the diagnosis of pancreatic cancer, a doctor may obtain a sample of the pancreas for examination under a microscope (biopsy) by inserting a needle through the skin using CT or an ultrasound scan as a guide. However, this approach sometimes misses the tumor. The same approach may be used to obtain a biopsy sample from the liver to look for cancer that has spread from the pancreas. If the results of these tests are normal but the doctor still strongly suspects adenocarcinoma, the pancreas may be evaluated surgically.
Endoscopic retrograde cholangiopancreatography (see figure Understanding Endoscopic Retrograde Cholangiopancreatography) is another test that may be done for people who have jaundice. Blood tests are also done.
Treatment of Pancreatic Cancer
Surgery
Chemotherapy or combination chemotherapy and radiation therapy (chemoradiation)
Pain relievers
The only hope of a cure is surgery, but surgery can be done only in people whose cancer has not spread. However, in most people, the tumor has already spread at the time of diagnosis. With surgery, either the pancreas and some of the first part of the small intestine (the duodenum) or just parts of the pancreas are removed.
Chemotherapy or chemoradiation may be given before surgery.
Because adenocarcinoma of the pancreas is fatal in most cases, a doctor usually discusses end-of-life care with the person, family members, and other health care professionals (see Treatment Options at the End of Life).
Prognosis for Pancreatic Cancer
Because adenocarcinoma of the pancreas has often spread to other parts of the body before it is discovered, the prognosis for pancreatic cancer is very poor. Fewer than 2% of people with adenocarcinoma of the pancreas survive for 5 years after the diagnosis.






