


Surgery is the term traditionally used to describe procedures (called surgical procedures) that involve manually cutting or stitching tissue to treat diseases, injuries, or deformities. However, advances in surgical techniques have made the definition more complicated. Sometimes lasers, radiation, or other techniques (other than scalpels) are used to cut tissue, and wounds may be closed without stitches.
In modern medical care, distinguishing between a surgical procedure and a medical procedure (usually thought of as a procedure that does not involve some cutting or stitching of tissue) is not always easy. However, making that distinction is not important as long as the doctor doing the procedure is well trained and experienced.
Surgery is a broad area of care and involves many different techniques. In some surgical procedures, tissue, such as an abscess or tumor, is removed. In other procedures, blockages are opened. In still other procedures, arteries and veins are attached in new places to provide additional blood flow to areas that do not receive enough.
In another surgical procedure called transplantation, organs such as the skin, kidney, or liver can be removed from the body and then transferred back into the same body (for example, with skin) or into a different body.
Grafts, sometimes made of artificial materials, may be implanted to replace blood vessels or connective tissue, and metal rods may be inserted into bone to stabilize or replace broken parts.
A diagnosis is sometimes accomplished by doing surgery. A biopsy, in which a piece of tissue is removed for examination under a microscope, is the most common type of diagnostic surgery. In some emergencies, in which there is no time for diagnostic tests, surgery is used for both diagnosis and treatment. For example, surgery may be needed to quickly identify and repair organs that are bleeding from injuries caused by a gunshot wound or motor vehicle crash.
The urgency of surgery is often described by three categories:
Emergency
Urgent
Elective
Emergency surgery, such as stopping rapid internal bleeding, is done as soon as possible because minutes can make a difference.
Urgent surgery, such as removal of an inflamed appendix, is best done within hours.
Elective surgery, such as replacement of a knee joint, can be delayed for some period of time until everything has been done to optimize a person's chances of doing well during and after the surgical procedure.
Cosmetic surgery
Cosmetic surgery is a type of elective surgery that is focused on enhancing appearance.
Cosmetic surgery involves a wide variety of operations, for example
Rhytidectomy: Removing wrinkles from the face and neck
Abdominoplasty: Removing fat and excess skin from the abdominal area
Mammoplasty: Enlarging or reducing breast size
Hair replacement surgery: Restoring scalp hair
Mandibuloplasty: Altering the appearance of the jaw
Blepharoplasty: Altering the appearance of the eyes
Rhinoplasty: Altering the appearance of the nose
Liposuction: Removing body fat
Sclerotherapy: Eliminating varicose veins
A person should choose a doctor who has met a medical specialty’s standards for practice (board certification) and who has extensive experience doing the operation.
Because obtaining the best results requires close adherence to instructions after the operation, cosmetic surgery is recommended only for highly motivated people.
Popular and tempting as cosmetic surgery may be, it is expensive and it poses risks, including serious health risks as well as the possibility that appearance may be less pleasing to the person than it was originally.
Anesthesia
Because surgery is typically painful, it is almost always preceded by the administration of some type of anesthetic, analgesic, or both. Anesthetics block the perception of pain by causing loss of sensation (numbness) or unconsciousness, and analgesics are drugs given to reduce pain. Anesthetics are typically given by health care practitioners specially trained and certified in providing anesthesia. These practitioners may be doctors (anesthesiologists) or nurse practitioners (nurse anesthetists). Nurse anesthetists practice under the direction of an anesthesiologist.
There are three types of anesthesia:
Local
Regional
General
Local anesthesia and regional anesthesia
In local anesthesia, the drug is injected under the skin of the site to be cut, numbing only that site.
In regional anesthesia, which numbs a larger area of the body, the drug is injected around one or more nerves and numbs an area of the body supplied by those nerves. For example, injecting a drug around certain nerves can numb fingers, toes, or specific parts or all of limbs. One type of regional anesthesia involves injecting a drug into a vein (intravenous regional anesthesia). A device such as a woven elastic bandage or blood pressure cuff compresses the area where the limb joins the body, trapping the drug within the veins of that limb. Intravenous regional anesthesia can numb an entire limb.
During local anesthesia and regional anesthesia, the person remains awake. However, doctors sometimes give mildly sedating antianxiety drugs intravenously to relax the person. Rarely, numbness, tingling, or pain can persist in the numbed area for days or even weeks after the surgical procedure.
Spinal anesthesia and epidural anesthesia are specific types of regional anesthesia in which a drug is injected around the spinal cord in the lower back. Depending on the site of the injection and position of the body, a large area (such as from the waist to the toes) can be numbed. Spinal and epidural anesthesia are useful for operations of the lower body, such as hernia repairs and prostate, rectal, bladder, leg, and some gynecologic operations. These types of anesthesia also can be useful for childbirth. Headaches occasionally develop in the days after spinal anesthesia but usually can be treated effectively.
General anesthesia
In general anesthesia, a drug that circulates throughout the bloodstream is given, making the person unconscious. The drug can be given intravenously or can be inhaled. Because a general anesthetic slows breathing, the anesthesiologist inserts a breathing tube in the windpipe. For short operations, however, such a tube may not be necessary. Instead, the anesthesiologist can support breathing by using a handheld breathing mask. If the operation is long, a ventilator breathes for the person ( see Mechanical Ventilation). General anesthetics affect vital organs, so the anesthesiologist closely monitors the heart rate, heart rhythm, breathing, body temperature, and blood pressure until the drugs wear off. Serious side effects are very rare.
Did You Know...
|
Major Surgery and Minor Surgery
A distinction is sometimes made between major surgery and minor surgery, but many surgical procedures have characteristics of both.
Major surgery
Major surgery often involves opening one of the major body cavities (abdomen, chest, and skull). Opening the abdomen is called laparotomy, opening the chest is called thoracotomy, and opening the skull is called craniotomy. Major surgery can stress vital organs. The surgery usually is done using general anesthesia in a hospital operating room by a team of doctors. A stay of at least one night usually is needed after major surgery, but some major surgical procedures are now being done safely in an outpatient setting, whether that is a hospital or a stand-alone ambulatory surgery center. Doctors consider many factors in determining whether a major surgical procedure can be done on an outpatient basis, including the person’s overall health and risk of complications, the complexity of the surgery, and whether a hospital is nearby in case the person needs to be transferred.
Minor surgery
In minor surgery, major body cavities are not opened. Minor surgery can involve the use of local, regional, or general anesthesia and may be done in an emergency department, an ambulatory surgical center, or a doctor's office. Vital organs usually are not stressed, and surgery can be done by a single doctor, who may or may not be a surgeon. Usually, the person can return home the same day that minor surgery is done.
Surgical Risk
The risks of surgery, that is, how likely surgery is to cause death or a serious problem, depend on the type of surgery and characteristics of the person.
Types of surgery that have the highest risk include
Heart or lung surgery
Liver surgery
Abdominal surgeries that take a long time to complete or have an increased risk of major bleeding
Prostate gland removal
Major operations on the bones and joints (for example, hip replacement)
Generally, the poorer the person's overall health, the higher the risks of surgery. Some particular health problems that increase surgical risk include
History of and risk factors for coronary artery disease
History of heart failure
History of stroke or transient ischemic attack
Symptoms of chest pain caused by coronary artery disease (angina)
Undernutrition (common among older people who live in institutions)
Severe disorders of the lungs or liver
Weakened immune system (for example, because of long-term corticosteroid treatment)
Risks are often higher among older people (see Spotlight on Aging: Surgical Risk and Age). However, risks are determined more by general health than by age. Chronic disorders that increase surgical risk and other treatable disorders, such as dehydration, infections, imbalances in body fluids and electrolytes, and particularly heart failure and angina, should be controlled with treatment as well as possible before an operation.
Second Opinion for Surgery
The choice to undergo surgery is not always clear. There may be nonsurgical options for treatment, and there may be several possible surgical procedures. Thus, a person may seek the opinion of more than one doctor ( see Getting a Second Opinion). Some health insurance plans require a second opinion for elective surgery. However, experts may disagree on which doctor should give the second opinion.
Some experts advise obtaining a second opinion from a doctor who is not a surgeon to eliminate any bias toward surgery when nonsurgical treatment is an option.
Other experts advise that another surgeon give the second opinion, believing that a surgeon knows more about the advantages and disadvantages of surgery than would a doctor who is not a surgeon.
Some experts recommend establishing up front that any surgeon giving a second opinion will not do the surgical procedure, so that there is no conflict of interest.
Surgery Through a Keyhole
Technical advances now make it possible to do surgery with smaller incisions and less tissue disruption than occurs with traditional surgery. To do this surgery, surgeons insert tiny lights, video cameras, and surgical instruments through keyhole-sized incisions. The surgeons can then do procedures using the images transmitted to video monitors as guides for manipulating the surgical instruments. In robotic surgery, the cameras provide surgeons with a three-dimensional view and surgeons control surgical instruments from a computer. Keyhole surgery has various names depending on where it is done: laparoscopy in the abdomen, arthroscopy in joints, and thoracoscopy in the chest. Because it causes less tissue damage than traditional surgery, keyhole surgery has several advantages, including the following:
However, the difficulties of keyhole surgery are often underestimated by people undergoing the surgery and sometimes by surgeons. Because surgeons are using a video monitor, they are seeing only a two-dimensional view of the site on which they are operating. Also, the surgical instruments used have long handles and are controlled from outside of the person’s body, so the surgeon may find that using them feels less natural than using traditional surgical instruments. For these reasons, keyhole surgery has potential disadvantages:
People also should know that although keyhole surgery may cause less pain than traditional surgery, pain still occurs, often more than anticipated. Because keyhole surgery is technically difficult, people should do the following:
|
Preparing for the Day of Surgery
Various preparations are made in the days and weeks before surgery. It is often recommended that physical conditioning and nutrition be improved as much as possible because good general health helps a person recover from the stress of surgery. Valuables should be left at home. Typically, people are told to not eat or drink anything after midnight the night before surgery.
Alcohol and drug use
Eliminating or minimizing alcohol use before undergoing surgery that involves general anesthesia can increase safety. Excessive alcohol consumption can damage the liver, causing heavy bleeding during surgery and unpredictably increasing or decreasing the effect of the drugs used for general anesthesia.
People who are dependent on alcohol or drugs may develop symptoms of withdrawal (see withdrawal symptoms of alcohol and also see withdrawal symptoms of drugs) when use of these substances is suddenly stopped or lessened before surgery. Therefore, doctors may give sedatives (benzodiazepines) to alcoholics on the day of surgery. Doctors may give opioid analgesics
Tobacco use
Smokers are advised to stop smoking as early as possible before any procedure involving the chest or abdomen. Recent tobacco use makes abnormal heart rhythms more likely to develop during general anesthesia and impairs lung function. People need to stop smoking several weeks before surgery so that the defense mechanisms of the respiratory system can recover.
Doctors' evaluations
The surgeon does a physical examination and takes a medical history, which includes the following:
Recent symptoms
Past medical conditions
Past reactions to anesthetics (if any)
Use of tobacco and alcohol
Infections
Risk factors for blood clots
Problems pertaining to the heart and lungs (such as cough or chest pain)
Allergies
or St. John’s wort) should be mentioned as well because they may have effects during or after surgery.
aspirin, 5 to 7 days before surgery. People may be told to continue taking other drugs that control chronic disorders, such as drugs used to lower blood pressure. Most drugs that are taken by mouth can be swallowed with a small sip of water on the day of surgery. Other drugs may have to be given by vein or delayed until after surgery.
The anesthesiologist may meet the person before the operation to review test results and identify any medical conditions that might affect the choice of anesthetic. The safest and most effective types of anesthesia may be discussed as well. The anesthesiologist also evaluates people who have a deviated septum or another airway abnormality before surgery that requires a breathing tube is done.
Tests
Depending on the person's overall health and the type of procedure, tests done before surgery (preoperative testing) may include blood and urine tests, an electrocardiogram, x-rays, and tests of lung capacity (pulmonary function tests). These tests can help determine how well the vital organs are functioning. If organs are functioning poorly, the stress of surgery or anesthesia can cause problems. Preoperative tests occasionally also reveal a hidden, temporary illness, such as an infection, which requires that surgery be delayed.
Blood storage for transfusion
People may wish to store their own blood in case a blood transfusion is needed during surgery. Using stored blood (autologous blood transfusion) eliminates the risk of infections and most transfusion reactions. A pint of blood at a time can be withdrawn from the person and preserved until surgery. Blood should be withdrawn no more often than once weekly, and the last withdrawal should probably be at least 2 weeks before surgery. The body replaces the missing blood during the weeks after the blood withdrawal.
Decision making
Sometime before the surgery, the surgeon obtains the person's permission to do the operation, a process called informed consent. The surgeon discusses risks and benefits of the operation, as well as alternative treatments, and answers questions. The person reads and signs a form documenting consent. In cases of emergency surgery in which the person is unable to provide informed consent, doctors try to contact the family. Rarely, emergency surgery must proceed before the family is contacted.
A durable power of attorney for health care and a living will should be prepared before surgery in case the person becomes unable to communicate or becomes incapacitated after surgery.
Preparing the digestive tract
Because some of the drugs given during surgery may cause vomiting, people should generally not eat or drink anything for at least 8 hours beforehand. For outpatient surgery, people should not eat or drink anything after midnight. Specific guidelines should be given and vary depending on the kind of surgery. People should ask the doctor which of their regularly prescribed drugs should be taken before surgery. People undergoing surgery involving the intestines are given laxatives or enemas for a day or two before the operation.
Fingernails
Because the device that monitors the level of oxygen in the blood is attached to a finger, nail polish and artificial nails should be removed before going to the hospital. Then, this device can perform more accurately.
The Day of Surgery
Before most operations, a person removes all clothing, jewelry, hearing aids, false teeth, and contact lenses or eyeglasses and puts on a hospital gown. The person is taken to a designated room (called the holding area) or to the operating room itself for final preparations before surgery. The skin that will be cut (operative site) is scrubbed with an antiseptic, which minimizes the number of bacteria and helps to prevent infection. A health care practitioner may remove hair from the operative site with clippers or with hair-removing liquids or creams.
Sometimes a plastic tube (catheter) is inserted into the bladder to collect urine during surgery.
A catheter is inserted in one of the veins of the hand or arm. Fluids and drugs are given through the catheter. A drug may be given by vein (intravenously) for sedation.
If an operation involves the mouth, intestinal tract, lungs or respiratory tract, or genitourinary tract, people are given one or more antibiotics within 1 hour before the operative site is cut to prevent infection (prophylaxis). Antibiotics are given by mouth or vein depending on the operation and are usually discontinued within 24 hours after surgery. This therapy also applies to people undergoing some other operations in which infections are particularly problematic (for example, joint or heart valve replacement).
Diabetes
On the day of surgery, people who use insulin
Dentures
Before a breathing tube is inserted in the windpipe, dentures must be removed. Ideally, before people are moved from the holding area, they should give their dentures to a family member.
Corticosteroids
The Operating Room
If the final preparations are done in the holding area, the person is then taken to the operating room. At this point, the person may still be awake, although groggy, or may already be asleep. The person is moved to the operating table, lit by specially designed surgical lights. Doctors, nurses, and other personnel who will be near or touching the operative site thoroughly scrub their hands with antiseptic soap, which minimizes the number of bacteria and viruses in the operating room. For surgery, they also wear scrub suits, caps, masks, shoe covers, sterile gowns, and sterile gloves. Before the surgery begins, a time out is held during which the surgical team confirms the following:
The person’s identity
The correct procedure and location and side of the operative site (if applicable)
Availability of all needed equipment
Verification that appropriate drugs to prevent problems such as infection or blood clots (if needed) were given
Local, regional, or general anesthesia is used.
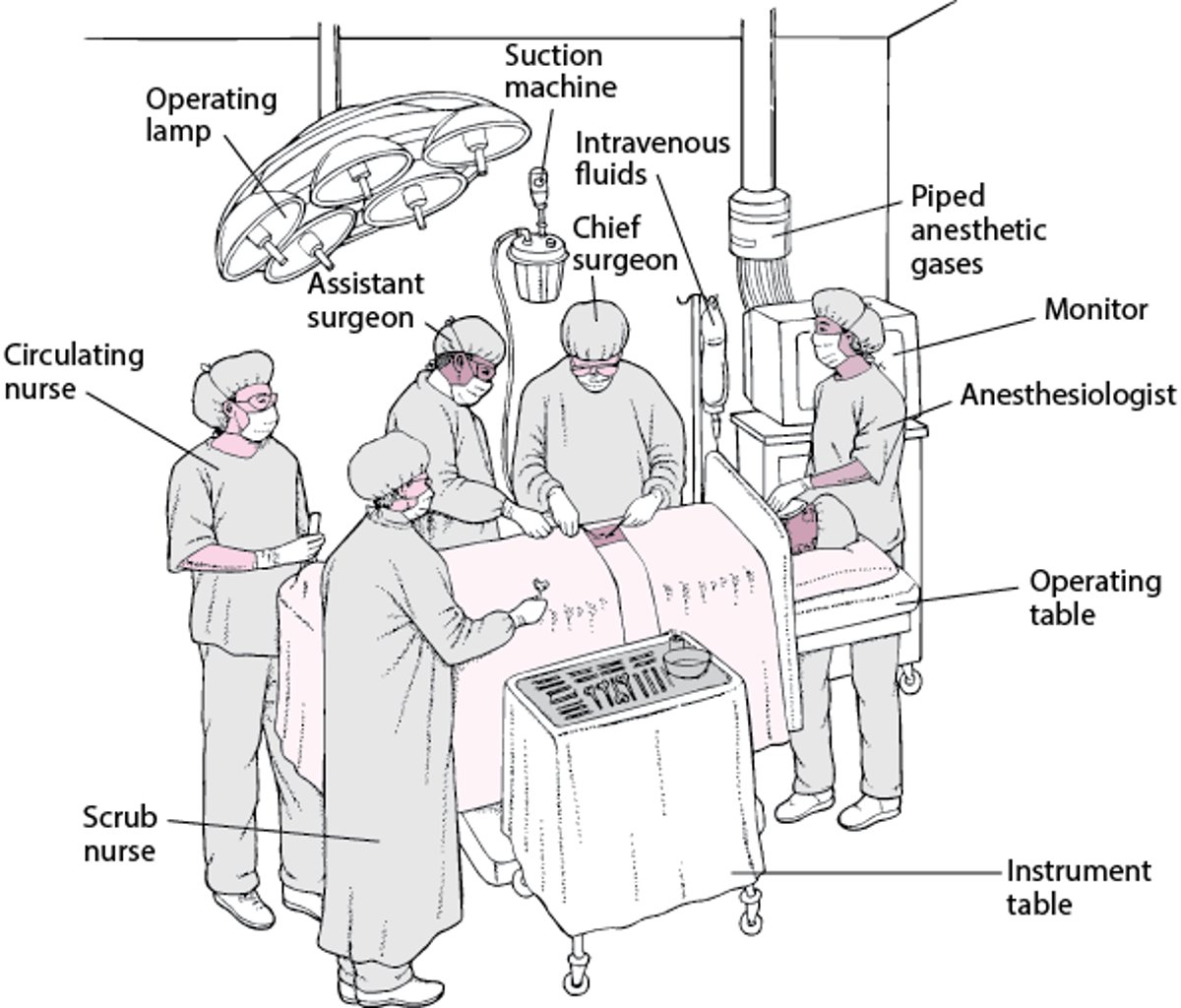
In the Operating Room
The operating room provides a sterile environment in which the operating team can do surgery. The operating team consists of the following:
The operating room typically contains a monitor that displays vital signs, an instrument table, and an operating lamp. Anesthetic gases are piped into the anesthetic machine. A catheter attached to a suction machine removes excess blood and other fluids, which can prevent surgeons from seeing the tissues clearly. Fluids given by vein, started before the person enters the operating room, are continued. |

After Surgery
After the operation is completed, the person is taken to a recovery room to be closely watched for about 1 or 2 hours while the anesthesia wears off. The care team makes sure the person is able to breathe, is not at risk of choking, and has drugs to control pain. The care team also evaluates whether the person is able to think clearly. Most people feel groggy when awakening, particularly after major surgery. Some people are nauseated for a short while. Some people feel cold.
Depending on the nature of the surgery and the type of anesthesia, a person may go home directly from the recovery room or be admitted to the hospital, sometimes in an intensive care unit (ICU).
Direct discharge home
A person being sent home must be
Thinking clearly
Breathing normally
Able to drink fluids
Able to urinate
Able to walk
Free of severe pain
People who had anesthesia or who have been given sedatives and then discharged need to be accompanied home by someone else and are not permitted to drive themselves. The operative site should be free of bleeding and unexpected swelling.
Hospitalization
People who are admitted to the hospital after surgery may awaken to find many tubes and devices in and on them. For example, there may be a breathing tube in the throat, adhesive pads on the chest to monitor the heartbeat, a tube in the bladder, a device attached to a finger to measure the level of oxygen in the blood, a dressing on the operative site, a tube in the nose or mouth, and one or more tubes in the veins.
Pain is expected after most operations and can almost always be relieved. Drugs that relieve pain (analgesics) can be given by vein (intravenously), by mouth, or by injection into the muscle or can be applied to the skin as a patch. If epidural anesthesia
Good nutrition is critical for healing and minimizing the chance of infection. Nutritional needs increase after major surgery. If surgery makes eating impossible for more than a week, an alternative source of nutrition may be needed. People whose digestive tracts are functioning but who are otherwise unable to eat may be given nutrients through a tube placed into the stomach. Such a tube may be passed through the nose, mouth, or an incision in the abdominal wall. Rarely, people who have had surgery of the digestive tract and cannot eat for extended periods may be given nutrients through a catheter inserted in one of the body’s large veins (parenteral nutrition).
Complications after surgery
Complications such as fever, blood clots, wound problems, confusion, difficulty urinating or defecating, muscle loss, and a deterioration in fitness (called deconditioning) can develop during the days after surgery.
Fever that develops during the days or weeks after surgery has several common causes, including the following:
Infections at the operative site
Lung problems such as pneumonia or collapsed lung tissue (called atelectasis)
Urinary tract infections (UTIs)
Blood clots in the legs (deep vein thrombosis [DVTs]) or lungs (pulmonary embolism)
Infections of devices, tubes, or drains that have been implanted
Drugs may sometimes cause fever. Another possible cause is inflammation in response to the trauma of an operation. The risk of infections at the operative site, DVTs, and UTIs can be decreased by meticulous care after surgery. The risk of pneumonia and atelectasis may be decreased by periodically breathing forcefully in and out of a handheld device (incentive spirometry) and coughing as needed.
Blood clots in the legs or pelvic veins (DVTs) occasionally develop after surgery, particularly if people lie immobile during and after surgery or have had surgery on their leg, pelvis, or both. The clots can dislodge and travel through the bloodstream to the lungs, where they can block blood from circulating through the lungs (causing pulmonary embolism). As a result, the oxygen supply to the rest of the body may be decreased, and sometimes blood pressure may fall.
Wound complications may include infection and separation of the wound edges (dehiscence). To decrease the risk of infection, doctors put a dressing on the surgical incision after surgery. The dressing placed in the operating room is typically left on for 24 to 48 hours unless signs of infection (such as increasing pain, swelling, and drainage) develop.
The dressing includes a sterile bandage and usually includes an antibiotic ointment. The bandage keeps bacteria away from the incision and absorbs fluids that ooze from the incision. Because these fluids can encourage bacteria to grow and infect the incision, the dressing is changed often, usually twice daily. The wound and any drainage tubes, sutures, or skin staples are examined whenever the dressing is changed, sometimes more often. Occasionally, infection develops despite the best wound care. An infected site becomes increasingly painful 1 or more days after surgery and can become red and warm or drain pus or fluid. Fever can develop. If any of these symptoms develop, the doctor should be seen as soon as possible.
Delirium (confusion and agitation) can develop, particularly among older people (see Spotlight on Aging: Surgical Risk and Age). Drugs with anticholinergic effects (such as confusion, blurred vision, and loss of bladder control— see Anticholinergic: What Does It Mean?), opioids, sedatives, or histamine-2 (H2) blockers may contribute, as may too little oxygen in the blood. Drugs that can cause confusion should be avoided in older people when possible.
Difficulty urinating and difficulty defecating
Loss of muscle (sarcopenia) and strength occur in all people who need bed rest for a long time. With complete bed rest, young adults lose about 1% of muscle per day, but older people lose up to 5% per day because they have lower levels of growth hormone, which is responsible for maintaining muscle tissue. Adequate amounts of muscle are important for recovery. Thus, people should sit up in bed, move, stand, and exercise as soon as and as much as is safe for them. People who are not receiving proper nutrition are at increased risk of sarcopenia. People are encouraged to eat and drink. If they are not able to eat and drink by themselves, tube feeding or, rarely, parenteral feeding may be necessary.
Discharge home after hospitalization (see also )
Before leaving the hospital, people are responsible for
Scheduling a follow-up visit with the doctor
Knowing what drugs to take
Knowing what activities to avoid or limit
Examples of activities that may need to be avoided temporarily include climbing stairs, driving a car, lifting heavy objects, and having sexual intercourse. A person should know what symptoms necessitate contacting the doctor before the scheduled follow-up visit.
Resuming normal activity during recovery from surgery should occur gradually. Some people need rehabilitation, which involves special exercises and activities, to improve strength and flexibility. For example, rehabilitation after hip replacement surgery can involve learning ways to walk, stretch, and exercise.
Spotlight on Aging: Surgical Risk and Age
In the mid-1900s, surgeons often hesitated to do even simple operations on people over age 50. Times have changed. Now, more than one third of all operations in the United States are done on people aged 65 or over. However, age does increase the risk of complications during and after surgery. For example, older people are much more likely than younger people to develop delirium after surgery. They are also more likely to have serious complications from bed rest, which may occur after surgery. These complications include
The risk of death during or after surgery also increases with age. More than three quarters of deaths in the period immediately after surgery occur in older people. Further, when emergency surgery is done or when surgery involves the chest or abdomen, the risk of death increases in all age groups, but much more so for the older age group. Although age itself is a risk factor, overall health and the presence of certain disorders increase surgical risk far more than age does. Having had a heart attack within 6 months of a surgical procedure greatly increases risk, as does poorly controlled heart failure. For example, heart failure, undernutrition (which is common among older people who live in institutions), and particularly severe or increasing chest pain (unstable angina) increase the risk of surgery in older people. Lung problems, such as chronic obstructive pulmonary disease, are of some concern when determining the risks of surgery, particularly among smokers. Impaired kidney function, type 1 diabetes, previous strokes or transient ischemic attacks, and problems with mental function, such as dementia, may also increase the risk. Certain surgical procedures pose more risk than others. For example, surgery involving the abdomen or chest, removal of the prostate, and major surgery on a joint (such as hip replacement) rank high on the list of risky procedures. Many procedures that older people commonly undergo, such as cataract surgery and surgery on small joints, pose lower risk. If an older person is generally well, most operations, including ones considered to be higher risk, can be done safely. When the risks of surgery are high, they still may be outweighed by the potential benefits. For example, surgery that involves some risk of death, such as repair of a large aortic aneurysm, should be considered if the person is expected to live for another 8 to 10 years because such aneurysms increase the risk of death if they are not repaired. However, such surgery should probably be avoided if other illnesses limit life expectancy to only 1 to 2 years. When the risks of surgery are low, the low risk may be outweighed by a lack of benefit. For example, some people believe that the risk of even more minor procedures (for example, a skin graft of a pressure sore), which usually is very low, is still much too great to justify putting a person with advanced dementia through such an operation. |




