


Occlusive peripheral arterial disease is blockage or narrowing of an artery in the legs (or rarely the arms), usually due to atherosclerosis and resulting in decreased blood flow.
Symptoms depend on which artery is blocked and how severe the blockage is.
To make a diagnosis, doctors measure blood flow to affected areas.
Medication, angioplasty, or surgery is used to relieve the blockage and reduce symptoms.
Occlusive peripheral arterial disease is common among older people because it often results from atherosclerosis (caused by buildup of plaque in the walls of the arteries), which becomes more common with aging.
Occlusive peripheral arterial disease is also common among
Men
People who have ever smoked regularly
People with diabetes, high blood pressure, abnormal cholesterol levels, or high blood homocysteine (a component of protein) levels
People who have a family history of atherosclerosis
People who are obese
People who are physically inactive
People who are older
Each of these factors contributes not only to the development of occlusive peripheral arterial disease but also to the worsening of the disease.
Occlusive peripheral arterial disease most commonly develops in the arteries of the legs (see Arteries of the Leg), including the two branches of the aorta (iliac arteries) and the main arteries of the thighs (femoral arteries), of the knees (popliteal arteries), and of the calves (tibial and peroneal arteries). Much less commonly, the disease develops in the arteries of the shoulders or arms.
Occlusive arterial disease may also develop in the part of the aorta that passes through the abdomen (abdominal aorta) or in its branches (see Abdominal Aortic Branch Occlusion).
Occlusive peripheral arterial disease may result from
Gradual narrowing of an artery
Sudden blockage of an artery
When an artery narrows, the parts of the body it supplies may not receive enough blood. An inadequate blood supply leads to insufficient oxygen levels in body tissues, which is called ischemia. Ischemia may develop suddenly or gradually. When an artery is suddenly or completely blocked, the tissue it supplies may die.

Gradual artery narrowing
Gradual narrowing of arteries is usually due to atherosclerosis, in which deposits of cholesterol and other fatty materials (atheromas or atherosclerotic plaques) develop in the walls of arteries. Atheromas may gradually narrow the interior (lumen) of the artery and reduce blood flow. Calcium, which is normally carried in the blood, may also accumulate in the walls of the blood vessels, making the arteries stiff and narrowing the artery.
Less commonly, arteries are gradually narrowed by an abnormal growth of muscle in the artery’s wall (fibromuscular dysplasia), inflammation (vasculitis), or pressure from outside the blood vessel by a nearby mass, such as a tumor or fluid-filled sac (cyst) that is expanding.
Sudden blockage of an artery
Sudden, complete blockage of an artery may result when a blood clot (thrombus) forms in an artery that is already narrowed. A sudden blockage may also result when a clot breaks off (becoming an embolus) from a site such as the heart or aorta, travels through the bloodstream, and lodges in an artery downstream.
Some disorders increase the risk of blood clot formation. They include atrial fibrillation, other heart disorders, and clotting disorders. Inflammation of blood vessels (vasculitis), which may be due to an autoimmune disorder, may also cause sudden blockage of an artery.
Sometimes an atheroma can rupture into the blood vessel and trigger the formation of a blood clot that suddenly blocks an artery. Other times, a piece of fatty material breaks off from an atheroma and suddenly blocks an artery. Sudden blockage may also result from an aortic dissection, in which the inner layer of the aorta tears, allowing blood to surge through the tear and separate the inner layer from the middle layer of the aorta. As the dissection enlarges, it can block one or more arteries connected to the aorta.
Symptoms of Occlusive Peripheral Arterial Disease
Symptoms of occlusive peripheral arterial disease vary depending on
Which artery is affected
How completely the artery is blocked
Whether the artery is gradually narrowed or suddenly blocked
Usually, about 70% of the artery’s interior has to be blocked before symptoms occur. Gradual narrowing of an artery may result in less severe symptoms than sudden blockage—even if the artery eventually becomes completely blocked. Symptoms may be less severe because gradual narrowing allows time for nearby blood vessels to expand or new blood vessels (called collateral vessels) to grow. Thus, the affected tissue can still be supplied with blood. If an artery is suddenly blocked, there is no time for collateral vessels to develop, so symptoms are usually severe.
Sudden, complete blockage of an artery in a leg or an arm may cause severe pain, coldness, and numbness in the affected limb. The person’s leg or arm is either pale or bluish (cyanotic) or with a distinct color change. No pulse can be felt below the blockage. The sudden, drastic decrease in blood flow to the limb is a medical emergency. The absence of blood flow can quickly result in loss of sensation in or paralysis of a limb. If blood flow is absent for too long, tissue may die, and the limb may need to be amputated.
Intermittent claudication, the most common symptom of peripheral arterial disease, results from gradual narrowing of a leg artery. It is a painful, aching, cramping, or tired feeling in the muscles of the leg—not in the joints. Intermittent claudication occurs regularly and predictably during physical activity but is always relieved promptly by rest. The muscles ache when a person walks, and the pain begins more quickly and is more severe when the person walks quickly or uphill. Usually, after 1 to 5 minutes of rest (sitting is not necessary), the person can walk the same distance already covered, although continued walking will again provoke the pain at a comparable distance. Most commonly, the pain occurs in the calf, but it can also occur in the thigh, hip, or buttock, depending on the location of the blockage. Very rarely, pain occurs in the foot.

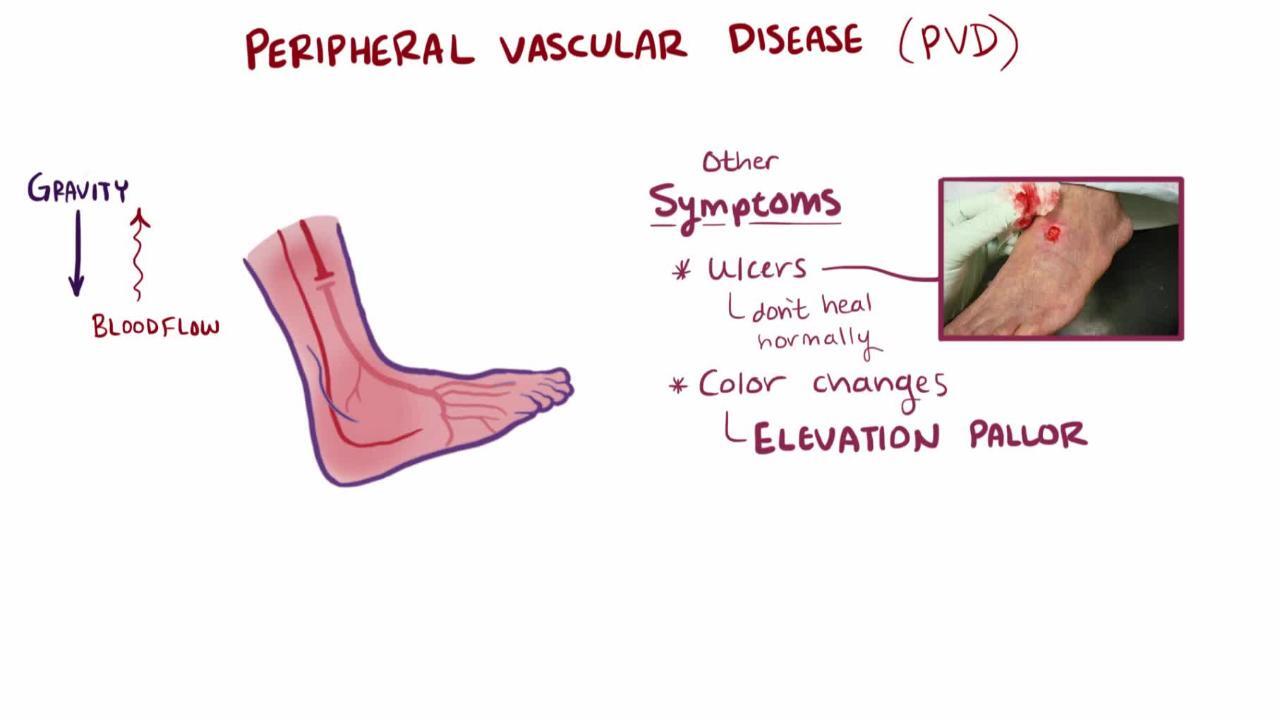
As a leg artery is narrowed further, the distance a person can walk without pain decreases. Eventually, as the disease becomes very severe, leg muscles may ache even at rest, especially when the person is lying down. Such pain usually begins in the lower leg or front of the foot, is severe and unrelenting, and worsens when the leg is elevated. The pain often interferes with sleep. For relief, the person may hang the feet over the side of the bed or rest sitting up with the legs hanging down.
Large blockages of the arm arteries, which are rare, may cause fatigue, cramping, or pain felt in the arm muscles when the arm is used repeatedly.


DR P. MARAZZI/SCIENCE PHOTO LIBRARY
When the blood supply is only mildly or moderately reduced, the leg or arm may look almost normal. When the blood supply to a foot is severely reduced, the foot may be cold, and doctors may need special equipment to detect pulses in the foot. The skin of the foot or leg may be dry, scaly, shiny, or cracked. Nails may not grow normally, and the hair on the leg may not grow. As the artery is narrowed further, a person may develop sores that do not easily heal, typically on the toes or heel and occasionally on the lower leg, especially after an injury. Infections occur easily and become serious quickly. In people with severe occlusive peripheral arterial disease, wounds in the skin may take weeks or months to heal or may not heal. Foot ulcers may develop. Leg muscles usually shrink (atrophy). A large blockage may cause gangrene (death of tissue due to lack of blood supply).
In some people who have had predictable, stable claudication, claudication can suddenly worsen. For example, calf pain that occurs after walking 10 blocks may suddenly occur after walking one block. This change may indicate that a new clot has formed in a leg artery. Such people should seek medical care immediately.
Did You Know...
|
Diagnosis of Occlusive Peripheral Arterial Disease
Physical examination and symptoms
Measurement of blood pressure and blood flow
Physical examination
The diagnosis of occlusive peripheral arterial disease is based on the symptoms and the results of a physical examination. Doctors examine the skin of the legs or arms, noting the color and temperature and pressing gently to see how quickly color returns after pressure is removed. These observations can help doctors determine whether circulation is adequate.
Procedures that directly measure blood pressure or blood flow are also done.

Blood pressure measurement is done using a standard blood pressure cuff and a special electronic stethoscope. The systolic blood pressure is measured in both arms and both legs. The pressure should be the same in the arms and legs. If blood pressure in the ankle is lower than that in the arms by a certain amount (less than 90% of arm pressure), blood flow to the legs is inadequate, and occlusive peripheral arterial disease is diagnosed. If doctors suspect a blockage in an arm artery, they measure systolic blood pressure in both arms. Pressure that is consistently higher in one arm suggests a blockage in the arm with lower blood pressure, and occlusive peripheral arterial disease is diagnosed.
Pulse assessment is also useful to assess blood flow. A doctor or nurse assesses each pulse, including those at the armpits, elbows, wrists, groin, ankles, and feet, and those behind the knees. The pulse in arteries beyond the blockage may be weak or absent. For example, if doctors suspect a blockage in a leg artery, they check the pulse below a certain point in the leg. For arteries in which the pulse is inaccessible, such as the renal arteries, procedures that provide images of blood flow are done. A stethoscope is used to listen for abnormal sounds caused by turbulent blood flow through a narrowed artery (bruits).
Tissue oxygen measurements
Transcutaneous oxygen tension testing measures the oxygen level of the tissue beneath the skin. Because oxygen is carried to the tissues by the blood, this test is an indirect measure of the blood flow. This painless test is done by placing sensors on the skin of the affected leg or arm and on the upper chest. Electrodes in the sensors heat the area underneath the skin to temporarily widen the blood vessels so that the oxygen level can be easily measured by the sensor.
Imaging
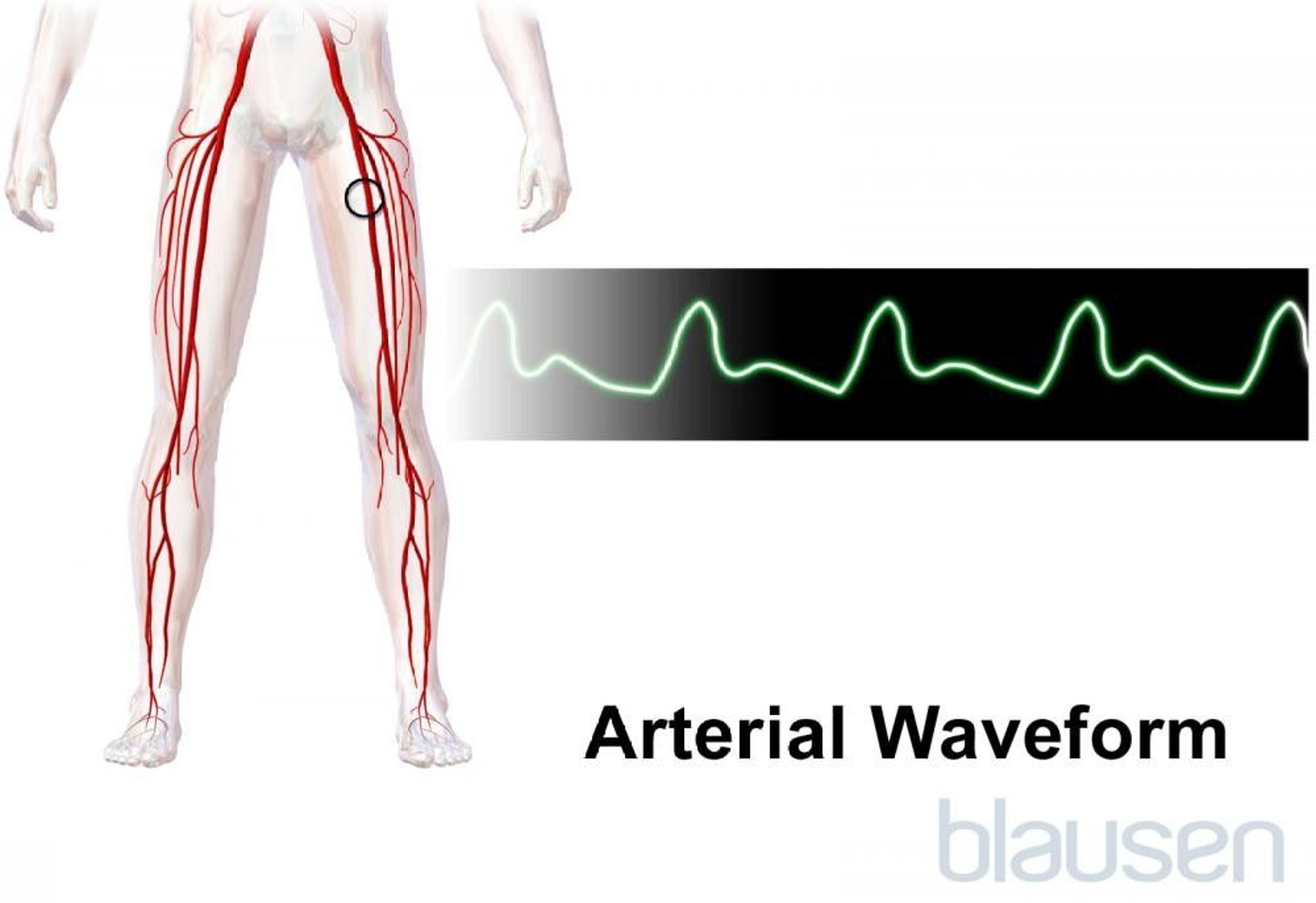
Doppler ultrasonography can be used to directly measure blood flow and can confirm the diagnosis of occlusive peripheral arterial disease. This procedure can accurately detect narrowing or blockage of blood vessels. Doppler ultrasonography to measure blood flow also may be done during exercise stress testing, because some problems appear only during exercise.
Usually, angiography, an invasive procedure in which a flexible plastic catheter is inserted into one of the large arteries in the upper thigh, is done only when surgery or angioplasty (opening up a blockage by inflating a small balloon within the artery) is required. In such cases, its purpose is to provide doctors with clear images of the affected arteries before surgery or angioplasty is done. Rarely, angiography is needed to determine whether surgery or angioplasty is possible. In angiography, a radiopaque contrast agent (dye), which can be seen on x-rays, is injected into an artery via the flexible plastic catheter. The contrast agent shows an outline of the inside of the artery when x-rays are done. Thus angiography can show the precise diameter of the artery and is more accurate than Doppler ultrasonography in detecting some blockages.
Most medical centers are doing angiography using a less invasive method such as computed tomography (CT angiography) or magnetic resonance imaging (called magnetic resonance angiography, or MRA). Rather than requiring an insertion of a flexible catheter into a major artery, these tests use small amounts of a contrast agent that are injected into the bloodstream by vein using a standard intravenous catheter in the arm.
Other tests for diagnosing occlusive peripheral arterial disease
For people with atherosclerosis, doctors try to identify risk factors, often by doing blood tests to measure levels of cholesterol, sugar (glucose), and, occasionally, homocysteine. Blood pressure is measured on more than one occasion to determine if it is consistently high.
Blood tests also may be done to identify other causes of narrowed or blocked arteries, such as inflammation of blood vessels due to an autoimmune disorder. Such blood tests include measuring the erythrocyte sedimentation rate (ESR) and level of C-reactive protein, which is produced only when inflammation is present. For blockage of an arm artery, doctors try to determine if the cause is atherosclerosis, thoracic outlet syndrome, or inflammation of the artery (arteritis).
Doctors may use magnetic resonance imaging (MRI) to rule out spinal stenosis (narrowing of the spinal canal), which can also cause pain during physical activity. However, this pain, unlike intermittent claudication, requires sitting, not just rest, for relief.
Treatment of Occlusive Peripheral Arterial Disease
Control risk factors
Exercise
Medications
Angioplasty
Surgery to relieve or bypass the blockage
Amputation of a limb if tissue dies
The aims of treatment are the following:
To prevent the disease from progressing
To reduce the risk of heart attack, stroke, and death due to widespread atherosclerosis
To prevent amputation
To improve the quality of life by relieving symptoms (such as intermittent claudication)
Treatments include medications such as those that relieve claudication and those that cause clots to dissolve (thrombolytic, or fibrinolytic, medications), angioplasty, surgery, and other measures, such as exercise and foot care. Which treatments are used depends on
Whether the blockage developed suddenly or gradually
The severity of the symptoms
The severity of the blockage
The location of the blockage
The risks related to the treatment (particularly for surgery)
The person's overall health
Regardless of the specific treatments used, people still need to treat disorders that are risk factors for atherosclerosis (such as high blood pressure, diabetes, and high cholesterol) and quit smoking to improve their overall prognosis. Angioplasty and surgery are only mechanical measures for correcting the immediate problem. They do not control or reverse the process that caused the disease in the first place.
Exercise
Regular exercise can help relieve the pain in most people with intermittent claudication. Exercise is the most effective treatment and may be appropriate for motivated people who can follow a prescribed daily exercise program. Exactly how exercise relieves claudication is not well understood, but exercise probably improves muscle function, improves blood flow, or causes new (collateral) blood vessels to grow. People with claudication should walk at least 30 minutes a day at least 3 times a week, if possible. For most people, following this routine increases the distance they can walk comfortably. Discomfort felt during walking is not dangerous. When discomfort is felt, a person should stop walking until the discomfort subsides and then walk again. The total walking time (excluding rest periods) must be at least 30 minutes to improve walking distance.
Exercise is usually most effective when it is supervised by a trained therapist in a rehabilitation program. Doctors recommend that people with claudication undergo an exercise stress test before they begin a rehabilitation program to make sure that the blood supply to heart muscle is adequate.
Foot care
Good foot care is important. It helps prevent wounds or foot ulcers from becoming infected and painful or resulting in gangrene. Good foot care also helps prevent amputation. Self-care measures include
Inspecting the feet daily for cracks, sores, corns, and calluses
Washing the feet daily in lukewarm water with mild soap, and drying them gently and thoroughly
Using unmedicated powder to keep the feet dry
Cutting toenails straight across and not too short (a podiatrist may have to cut the nails; the podiatrist needs to know that the person has peripheral arterial disease)
Having a podiatrist treat corns or calluses
Avoiding adhesive or harsh chemicals to remove corns or calluses
Changing socks or stockings daily and shoes often
Wearing loose wool socks to keep the feet warm
Not wearing tight garters or stockings with tight elastic tops
Wearing shoes that fit well and have wide toe spaces
Avoiding open shoes or walking barefoot
Asking the podiatrist about a prescription for special shoes if the feet are deformed
Not using hot water bottles or heating pads
Not soaking feet in hot water or chemical solutions
Foot ulcers require meticulous care. Such care is needed to treat infection, to protect the skin from further damage, and to enable the person to continue to walk.
A foot ulcer must be kept clean. It should be washed daily with a mild soap or antibacterial solution and covered daily with clean, dry dressings. The legs should be kept below the level of the heart to help improve blood flow. People with diabetes must control blood sugar levels as well as possible. As a rule, anyone with poor circulation to the feet or with diabetes should have a doctor check a foot ulcer that is not healing after about 7 days. Often, doctors prescribe an antibiotic ointment.
If foot ulcers are not healing, a person may need complete bed rest. If bed rest is required, bandages with heel pads or foam-rubber booties should be worn to prevent bedsores (pressure sores) from developing on the feet. The head of the bed should be raised 6 to 8 inches (about 15 to 20 centimeters) and the legs kept at or below heart level, so that gravity helps blood flow through the arteries. If the ulcer is infected, doctors usually prescribe antibiotics to be taken by mouth, and the person may need to be hospitalized.
Medications
Aspirin or clopidogrel
A class of drugs called angiotensin-converting enzyme inhibitors, helps blood vessels dilate and sometimes improve blood flow.
Angioplasty
Angioplasty to widen a blood vessel is sometimes done immediately after angiography. When a blockage occurs suddenly, angioplasty must be done as soon as possible to prevent irreversible loss of limb function or amputation. Angioplasty may be done to relieve symptoms and thus postpone or avoid surgery. Sometimes it is used in combination with surgery or a procedure to remove a blood clot.
Angioplasty consists of inserting a catheter with a balloon at its tip into the narrowed part of the artery and then inflating the balloon to clear the blockage. To keep the artery open, doctors may insert a permanent wire mesh (a stent) into the artery. Some stents contain drugs that are slowly released (drug-eluting stents) and prevent recurrence of the blockage.
Angioplasty is usually done as an outpatient procedure. Angioplasty is rarely painful but may be somewhat uncomfortable because the person has to lie still on a hard table. A mild sedative, but no general anesthetic, is given.
The success of angioplasty varies, depending on the location of the blockage and the severity of peripheral arterial disease. Afterward, the person is given medication (such as aspirin
Angioplasty cannot be done successfully if too many areas of an artery are narrowed, the narrowed section is too long, or the artery is severely and extensively hardened.
After angioplasty, surgery may be needed if a blood clot (thrombus) forms in the narrowed area, if a piece of the clot (embolus) breaks off and blocks an artery downstream, if blood seeps into the lining of the artery causing a bulge inward that blocks blood flow (a disorder called dissection), or if severe bleeding occurs.
Other devices—including lasers, mechanical cutters, ultrasonic catheters, and rotational sanders—can be used instead of a balloon catheter during angioplasty, but none appears to be more effective.
Surgery
Surgery to remove the blockage or bypass surgery (see figure Bypass Surgery in the Leg) may be done if other treatments do not relieve claudication. Surgery is usually done to avoid amputation of a leg when blood flow is greatly reduced—that is, when claudication is incapacitating or occurs during rest, when wounds do not heal, or when gangrene develops.
Surgery to remove blood clots (thromboendarterectomy) can be done when thrombolytic medications are ineffective in dissolving the clot or too dangerous. Surgery to remove atheromas (endarterectomy) or other blockages may also be done.
Bypass Surgery in the Leg
Bypass surgery may be done to treat arteries that are narrowed or blocked. In this procedure, blood is rerouted around the affected artery—for example, around part of the femoral artery in the thigh or part of the popliteal artery in the knee. A graft consisting of a tube made of a synthetic material or part of a vein from another part of the body is joined to the blocked artery above and below the blockage. |

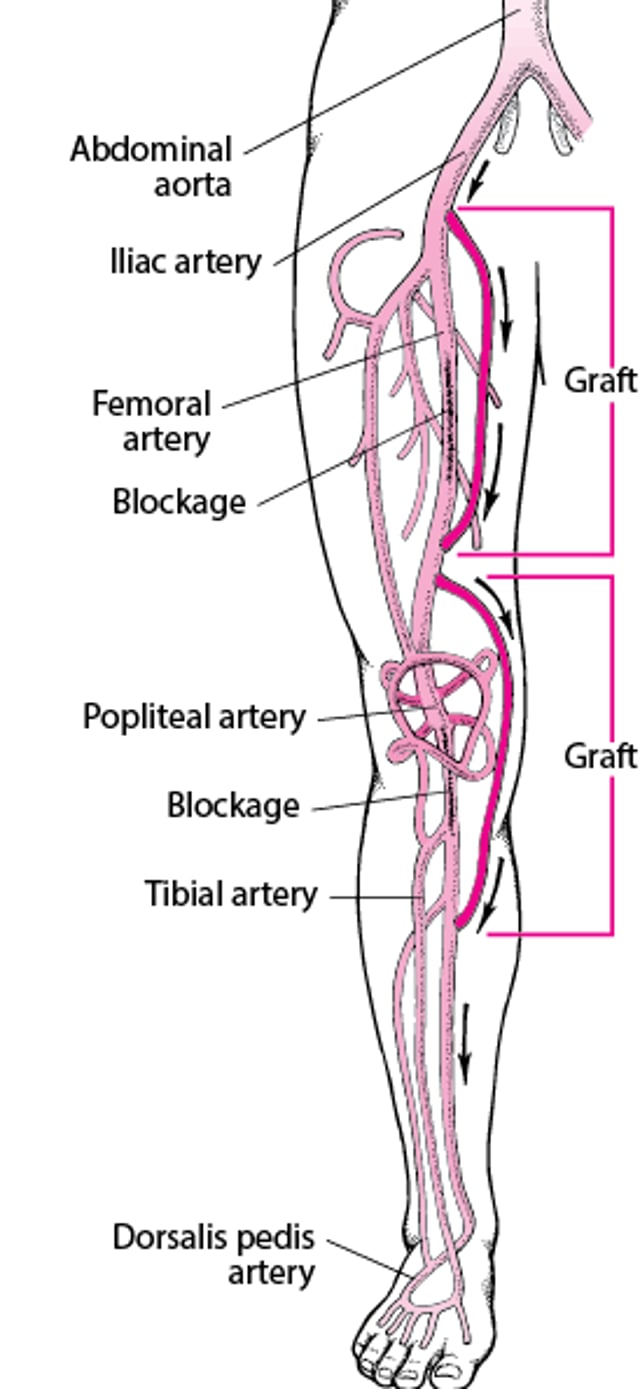
Alternatively, bypass surgery may be done. In bypass surgery, a graft consisting of a tube made of a synthetic material or a part of a vein from another part of the body is joined to the blocked artery above and below the blockage. Thus, blood is rerouted around the blocked artery.
Another approach is to remove the narrowed or blocked section and insert a graft in its place. Usually before surgery, doctors assess heart function and blood flow through the heart to determine the relative safety of surgery, because many people with occlusive peripheral arterial disease also have coronary artery disease.
Rarely, amputation of the leg is required if part of a limb has died or if there is no good way to restore blood flow to the area. Amputation is done to remove infected tissue, relieve unrelenting pain, or stop worsening gangrene. Surgeons remove as little of the leg as possible. Preserving the knee is particularly important if the person plans to wear an artificial leg. Physical rehabilitation after leg amputation is important.
Other treatments
Exposure to cold, which causes blood vessels to narrow (constrict) and further restricts the blood reaching the tissue, should be minimized.
cocaine and amphetamines.
The injection of stem cells into the legs of people with severe deficiencies in blood flow is currently being studied. Stem cells may stimulate the growth of new blood vessels, thereby reducing the need for amputation.
Prevention of Occlusive Peripheral Arterial Disease
The best way to help prevent occlusive peripheral arterial disease is to modify or eliminate risk factors for atherosclerosis. Prevention includes the following measures:
Controlling diabetes
Lowering high blood pressure and high cholesterol levels
Losing weight
Engaging in regular physical activity
Sometimes, taking medications to prevent complications such as coronary artery disease
Good control of diabetes, high blood pressure, and high cholesterol levels helps delay or prevent the development of occlusive peripheral arterial disease and reduces the risk of other complications.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American Heart Association: Peripheral Arterial Disease Resources: Comprehensive information for people living with peripheral arterial disease, including information about symptoms and treatment






