


Giant cell arteritis is chronic inflammation of large and medium arteries of the head, neck, and upper body. Typically affected are the temporal arteries, which run through the temples and provide blood to part of the scalp, the jaw muscles, and the optic nerves.
The cause is unknown.
Typically, people have a severe and often throbbing headache, pain in the scalp when they brush their hair, and pain in facial muscles when they chew.
Without treatment, blindness can result.
Symptoms and results of a physical examination suggest the diagnosis, but biopsy of the temporal artery is done to confirm it.
(See also Overview of Vasculitis.)
Giant cell arteritis is a relatively common form of vasculitis in the United States and Europe. Women are affected more often than men. Giant cell arteritis typically affects people over age 55, often at about age 70. About 40 to 60% of people with giant cell arteritis also have symptoms of polymyalgia rheumatica. The cause of these disorders is unknown.
Symptoms of Giant Cell Arteritis
Symptoms of giant cell arteritis may begin gradually over several weeks or abruptly. People may have fever and feel tired and generally unwell. They may lose weight unintentionally and sweat more than usual. Symptoms vary, depending on which arteries are affected.
Headache and scalp pain
Typically, the large arteries to the head are affected, causing a severe, sometimes throbbing headache at the temples or back of the head to develop for the first time. Arteries in the temple may be tender to the touch and feel swollen and bumpy. The scalp may feel painful when touched or when the hair is brushed.
Blindness and visual disturbances
Double or blurred vision, large blind spots, sudden blindness in one eye that resolves within a few minutes, or other eye problems may develop. The greatest danger is permanent blindness, which can occur suddenly if the blood supply to the optic nerve is blocked. Complete blindness in both eyes is uncommon if people are treated as soon as the diagnosis is suspected but can occur without treatment. Over the past 50 years, the number of visual disturbances has gone down while recovery rates have gone up, most likely because giant cell arteritis is diagnosed earlier and treated before the eyes are affected.
Jaw and tongue pain
Typically, the jaw muscles hurt and become tired soon after people begin chewing. The tongue may also hurt when eating or speaking. People who experience pain in the jaw and tongue are more likely to have visual problems.
Neurologic and cardiovascular problems
Occasionally, blood flow to the brain is blocked, and a stroke occurs.
Sometimes inflammation damages the aorta, causing its lining to tear (dissection) or a bulge (aneurysm) to form in its wall.
If polymyalgia rheumatica is also present, severe pain and stiffness may occur in the neck, shoulders, and hip that is worse during the night and in the morning.
Did You Know...
|
Diagnosis of Giant Cell Arteritis
A doctor's evaluation
Blood tests
Biopsy of the temporal artery
Sometimes, ultrasound of the temporal arteries
Doctors suspect the diagnosis of giant cell arteritis based on symptoms and results of a physical examination. Doctors feel the temples to see whether the temporal arteries feel hard, bumpy, or tender.
Blood tests are done. Results can support the diagnosis. For example, anemia, a very high erythrocyte sedimentation rate (ESR), and a high level of C-reactive protein indicate inflammation.
A biopsy of the temporal artery (in the temple) is often done to confirm the diagnosis.
Another test to help confirm the diagnosis is an ultrasound of the temporal arteries. It can sometimes make a biopsy unnecessary.
The diagnosis is also more likely if the patient also has symptoms of polymyalgia rheumatica.
If giant cell arteritis is suspected in very large arteries, such as the aorta and its major branches, magnetic resonance angiography may be done to confirm the diagnosis.
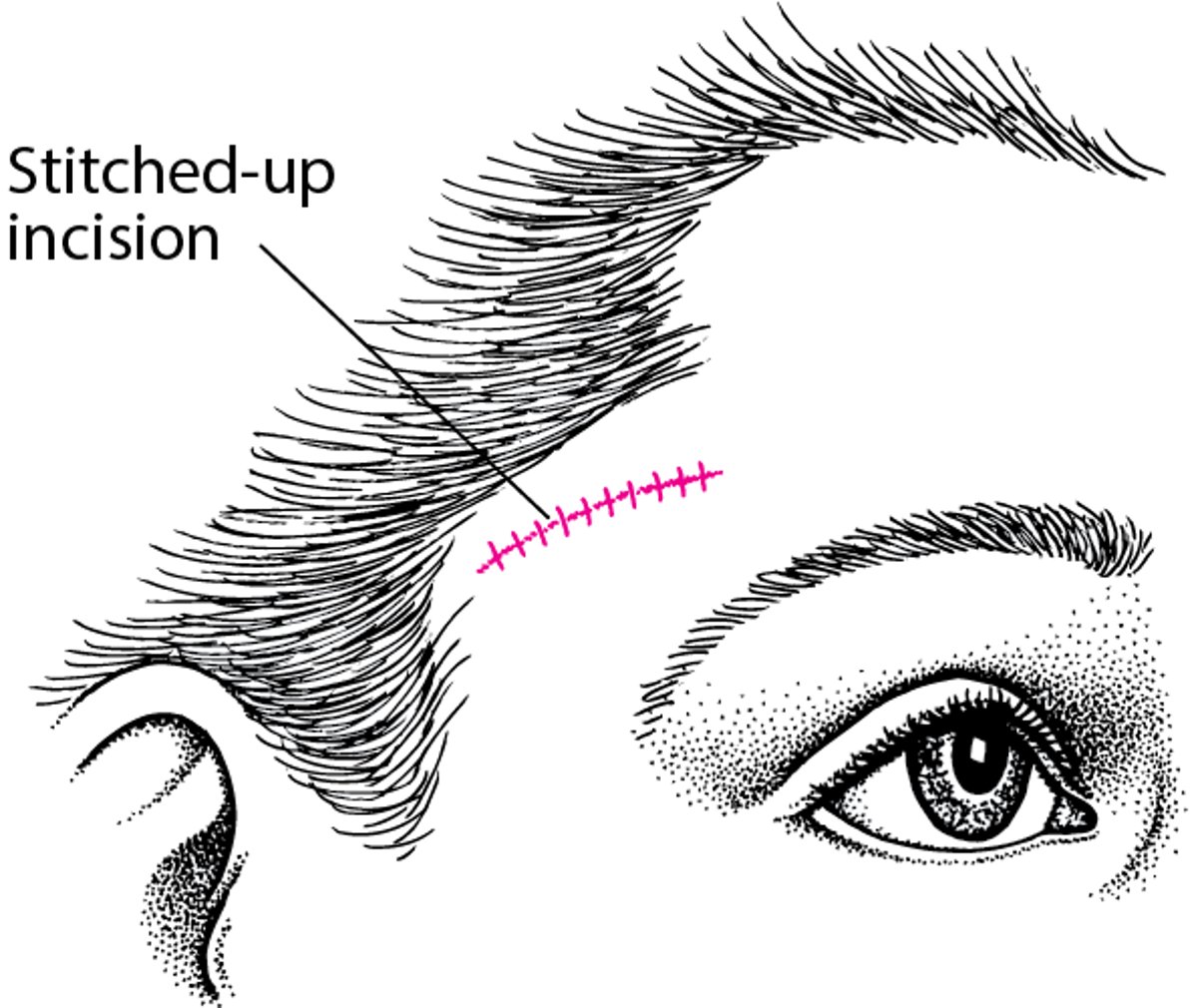
Biopsy of the Temporal Artery
A biopsy of the temporal artery is the definitive procedure for diagnosing temporal arteritis. Doppler ultrasonography is occasionally used to locate the part of the temporal artery to be biopsied. After a local anesthetic is injected, a shallow incision is made directly over the artery, and a segment of the artery at least 1 inch long is removed. The incision is then stitched up. |

Treatment of Giant Cell Arteritis
With treatment, most people with giant cell arteritis recover fully, but the disorder may return.
Treatment of giant cell arteritis is started as soon as the disorder is suspected because, without treatment, blindness can develop. Treatment is usually started even before a biopsy is done. Treatment does not affect the biopsy results as long as the biopsy is done within 2 weeks after starting treatment.
Spotlight on Aging: Giant Cell Arteritis and Polymyalgia Rheumatica
Giant cell (temporal) arteritis and polymyalgia rheumatica, which often occur together, affect people over age 55 almost exclusively. These disorders become more common as people age. They are 10 times more common among people over age 80 than among those aged 50 to 59. Giant cell arteritis typically causes a throbbing headache and problems with vision (including pain in and around the eyes). Polymyalgia rheumatica makes muscles painful and stiff. Without treatment, the pain these disorders cause, whether they occur together or separately, can make everyday living miserably difficult. Also, without prompt treatment, giant cell arteritis can cause blindness. The main treatment of these disorders, corticosteroids, may be problematic in older people. These drugs can cause dramatic improvement and are essential for preventing blindness. However, they are more likely to have side effects in older people. People may retain fluids, their appetite may increase, and they may become confused. Blood sugar may increase, sometimes causing diabetes, and bone density may decrease. Blood pressure may increase. To reduce the risk of these effects, doctors reduce the dose of the corticosteroid and stop the drug as soon as possible. Older people who take corticosteroids are encouraged to take measures to help maintain bone density. They can do weight-bearing exercise and take . Taking antiresorptive drugs can help increase bone density. Such drugs include bisphosphonates Faithfully continuing treatment as instructed results in complete recovery for many people. |
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
Vasculitis Foundation: Provides information for patients about vasculitis, including how to find a doctor, learn about research studies, and join patient advocacy groups






