




Sleep is necessary for survival and good health, but why sleep is needed and exactly how it benefits people are not fully understood. One of sleep's benefits is its restorative effect on people's ability to function normally during the daytime.
Individual requirements for sleep vary widely, usually from 6 to 10 hours every day. Most people sleep at night. However, many people must sleep during the day to accommodate work schedules—a situation that can lead to sleep disorders.
Did You Know...
|
How long people sleep and how rested they feel after waking can be influenced by many factors, including the following:
Level of excitement or emotional distress
Age
Diet
Use of drugs
For example, some drugs make people sleepy, and others make sleeping difficult. Some food components or additives, such as caffeine, strong spices, and monosodium glutamate (MSG), may disturb sleep. Older adults tend to fall asleep earlier, to awaken earlier, and to be less tolerant of changes in sleep habits.
Snoring may interfere with sleep—the snorer's or the snorer's bed partner's.


The sleep cycle
All sleep is not the same. There are 2 main types of sleep:
Rapid eye movement (REM) sleep
Nonrapid eye movement (NREM) sleep, which has 3 stages
People normally cycle through the 3 stages of NREM sleep (stages N1 through N3), usually followed by a brief interval of REM sleep, every 90 to 120 minutes or several times every night. Throughout the night, people wake up briefly (called stage W) but are typically unaware of being awake.
NREM sleep: NREM sleep accounts for about 75 to 80% of total sleep time in adults. Sleep progresses from stage 1 (the lightest level, when the sleeper can be awakened easily) to stage 3 (the deepest level, when the sleeper can be awakened with greater difficulty). In stage 3, blood pressure is at its lowest, and heart and breathing rates are at their slowest. People perceive stage 3 as high-quality sleep.
REM sleep: Electrical activity in the brain is unusually high, somewhat resembling that during wakefulness. The eyes move rapidly, and certain muscles are paralyzed so that voluntary movement is impossible. However, some muscles may twitch involuntarily. The rate and depth of breathing increase.
The most vivid dreaming occurs during REM sleep. Most talking during sleep, night terrors, and sleepwalking occur during stage 3 NREM sleep.
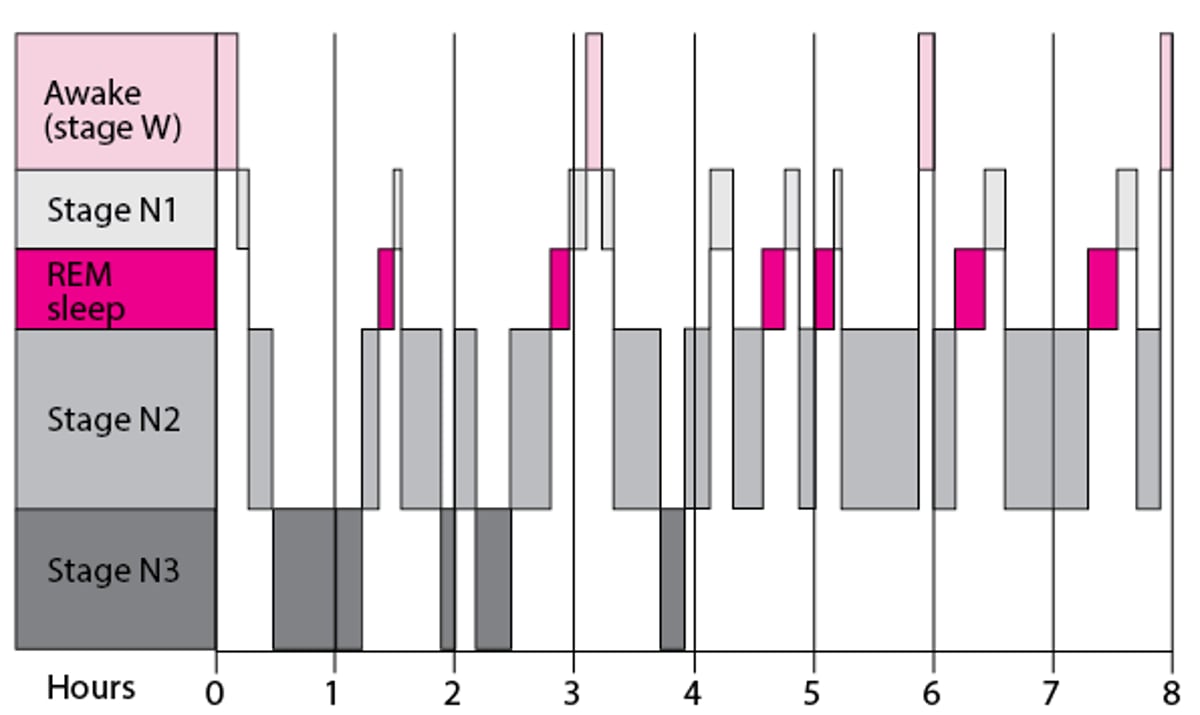
Stages of the Sleep Cycle
People normally cycle through distinct stages of sleep every 90 to 120 minutes during the night: 3 stages of nonrapid eye movement sleep (N) and 1 stage of rapid eye movement (REM) sleep. Relatively little time is spent in stage N1 (shallow) sleep. The greatest time is spent in stage N2 sleep. Deep sleep (stage N3) occurs mostly during the first half of the night. More time is spent in REM sleep as the night progresses. Brief awakenings (called stage W) occur throughout the night, but the sleeper is typically unaware of most of them. |

Sleep disorders
Almost half of all people in the United States report problems with sleeping. (See also Sleep Problems in Children.)
Sleep disorders involve disturbances in the ability to fall asleep, stay asleep, or stay awake or unusual behaviors during sleep, such as sleepwalking. Sleep can be disturbed by many factors, including irregular bedtimes, activities before bed, stress, diet, disorders, and drugs.
The most common symptoms of sleep disorders are
Insomnia can be a disorder or a symptom of another disorder. Excessive daytime sleepiness is not a disorder but a symptom of various sleep-related disorders.
People with insomnia have difficulty falling and staying asleep and usually wake up feeling unrefreshed. They may wake up early. Lack of sleep makes people feel sleepy, tired, and irritable during the day.
People with excessive daytime sleepiness tend to fall asleep during normal waking hours. Some sleep disorders make people unable to resist falling asleep during the day.
Some sleep disorders involve involuntary movements of the limbs or other unusual behaviors (such as nightmares, night terrors, or sleepwalking) during sleep. Unusual movements and behaviors during sleep are called parasomnias.
Other symptoms may include problems with memory, coordination, and emotions. People may perform less well in school or at their jobs. The risk of having a motor vehicle accident or developing a heart disorder is increased.
A detailed description of the problem, sometimes with information from a sleep log, usually indicates the diagnosis, but sometimes testing in a sleep laboratory is needed. This testing includes polysomnography.
Essentials for Older Adults: Sleep
Up to half of older adults say that they do not sleep as well as they would like. As people age, total sleep time and deep sleep tend to decrease, and sleep is more likely to be interrupted.
Although causes of poor sleep may be the same as for younger adults, age-related changes may also contribute to poor sleep.
Age-related changes
As people age, they may participate in fewer activities and become less physically active, making falling asleep and staying asleep harder.
If older people have to move into a relative’s home or a nursing home, they may have no control over such things as temperature and noise levels. The resulting discomfort can make sleeping more difficult.
Older adults may go out less and spend less time outdoors, reducing their exposure to sunlight. If the eyes are not exposed to enough sunlight, the body's internal (biologic) clock may become out of sync with the earth’s cycle of light and dark. Then, people may have difficulty sleeping when they are supposed to (at night).
Also, as people age, the body produces less melatonin and growth hormone. This change affects sleep because both of these hormones promote deep sleep.
Older adults are more likely to fall asleep and wake up early than are younger adults and children. Compared with younger people, older adults also spend less time in deep sleep (which may help the body recover from daytime activities). Once asleep, they wake up more often and more easily. As a result, they feel less refreshed when they wake up, even though they may have spent a long time in bed. Usually, these changes alone do not indicate a sleep disorder in older adults, but they may indicate a disorder if the changes make it difficult for people to function during the day.
Older adults tend to be less tolerant of changes in sleep habits. For example, they may be more prone to jet lag and problems related to shift work.
Disorders in older adults
Older adults are more likely to have medical and emotional disorders that can interfere with sleep.
Disorders interfere with sleep in several ways:
By causing pain (as occurs in arthritis)
By making breathing difficult (as occurs in heart or lung disorders or obstructive sleep apnea)
By making people have to urinate more often, waking them up frequently during the night (as occurs in benign prostatic hyperplasia, diabetes, and heart failure)
Depression, which is common among older adults, also interferes with sleep.
Medications in older adults
Older adults are more likely to take medications that affect sleep. Some (such as diuretics for heart failure) increase the need to urinate and thus interrupt sleep. Other medications make people sleepy during the day or stimulate them. Either way, sleeping at night may be harder.
Medications to aid sleep (hypnotics), whether prescribed by a doctor or available over-the-counter (OTC), even in small doses, can have side effects These side effects are more likely to occur in and cause more problems in older adults. They can include daytime drowsiness, clumsiness, nervousness, agitation, difficulty urinating, and confusion. These medications also increase the risk of falls during the night.
Older adults and napping
Older adults tend to take naps because they do not sleep well during the night. Napping during the day may help compensate for not sleeping during the night, but it may also make sleeping at night more difficult. Napping may be more likely because the aging body is less able to regulate blood pressure as needed. For example, after a big meal, blood pressure decreases, and the body needs to pump relatively more blood to the head. The aging body is less able to make this adjustment. As a result, older adults lie down more, sometimes resulting in a nap.
Measures to improve sleep in older adults
Generally, older adults need as much sleep as they did when they were young and should not accept poor sleep as part of aging. They can take measures to improve sleep, such as the following:
Stay active but refrain from exercise and excitement late in the evening.
Spend time outside.
Avoid foods and beverages (such as those that contain caffeine or alcohol) that can interfere with sleep or only drink caffeinated beverages early during the day.
Make sure that their bedroom is conducive to sleep (that is, cool and dark).
Go to bed and—more importantly—wake up at regular times.







