


Because different areas of the brain control specific functions, the location of brain damage determines the type of dysfunction that results.
Parts of the Brain

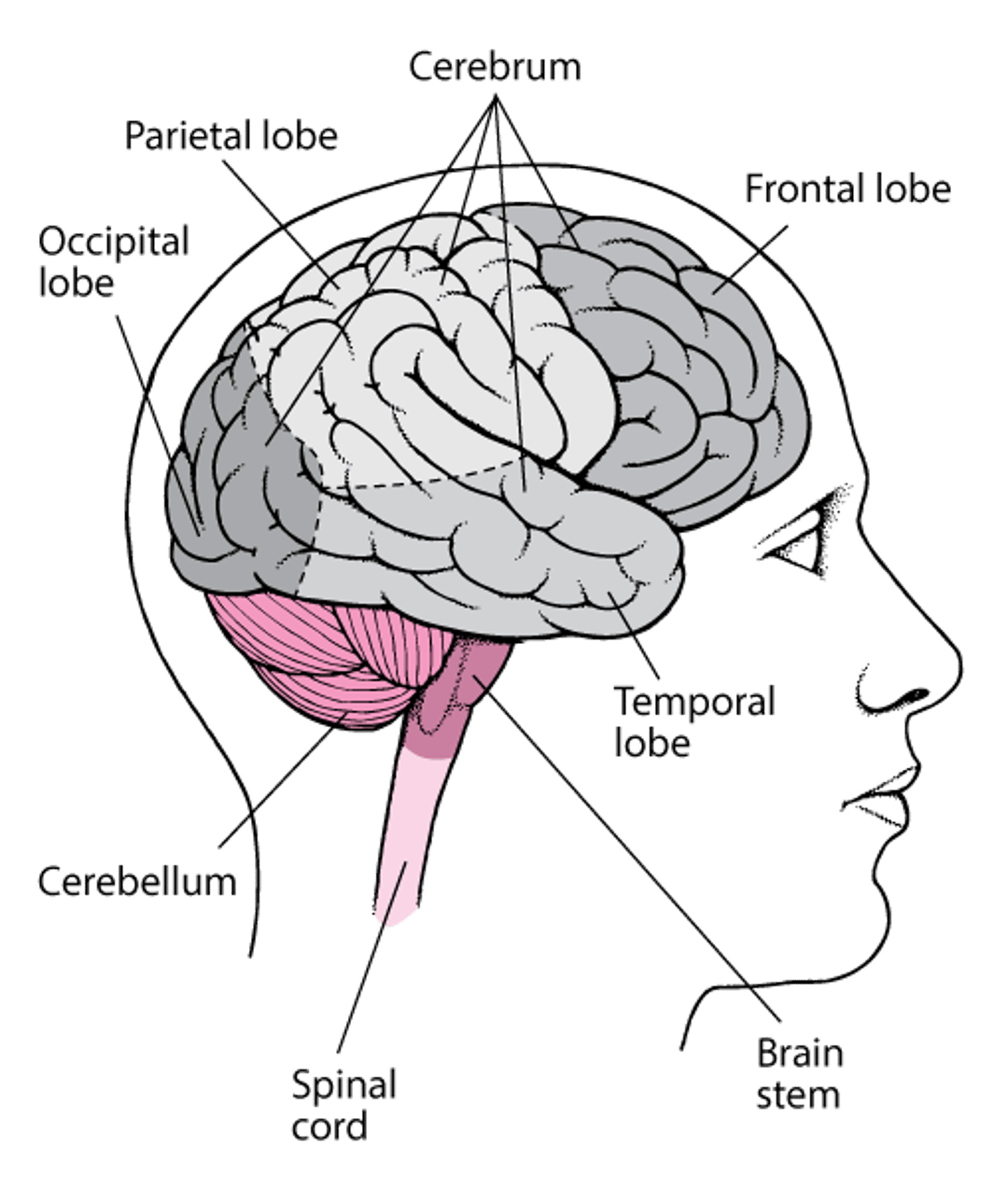
Which side of the brain is affected is also important because the functions of the two halves of the cerebrum (cerebral hemispheres) are not identical. Some functions of the brain are performed exclusively by one hemisphere. For example, movement and sensation on one side of the body are controlled by the hemisphere on the opposite side. Other functions are performed mainly by one hemisphere, which is said to be dominant for that function, and the other hemisphere is said to be nondominant. For example, the left hemisphere mainly controls language in most people. This characteristic is called left-hemisphere language dominance. Damage to only one hemisphere of the brain may cause complete loss of such functions.
However, most functions (such as memory) require coordination of several areas in both hemispheres. For such functions to be completely lost, both hemispheres must be damaged.
Specific patterns of dysfunction can be related to the area of the brain that has been damaged.
Usually, doctors can diagnose the type of dysfunction by examining the person. They ask questions designed to evaluate specific brain functions. Imaging tests, such as computed tomography (CT) and magnetic resonance imaging (MRI), are usually needed to identify the cause of the damage.
Frontal Lobe Damage
The frontal lobes have the following functions:
Initiating many actions
Controlling learned motor skills, such as writing, playing musical instruments, and tying shoelaces
Controlling complex intellectual processes, such as speech, thought, concentration, problem-solving, and planning for the future
Controlling facial expressions and hand and arm gestures
Coordinating expressions and gestures with mood and feelings
Generally, damage to the frontal lobes causes loss of the ability to solve problems and to plan and initiate actions, such as crossing the street or answering a complex question (sometimes called executive functions). But some specific impairments vary depending on which part of the frontal lobe is damaged.
If the back part of the frontal lobe (which controls voluntary movements) is damaged, weakness or paralysis can result. Because each side of the brain controls movement of the opposite side of the body, damage to the left hemisphere causes weakness on the right side of the body, and vice versa.
If the middle part of the frontal lobe is damaged, people may become apathetic, inattentive, and unmotivated. Their thinking becomes slow, and their responses to questions are very slow.
If the middle back part of the left frontal lobe (Broca area) is damaged, people may have difficulty expressing themselves in words—an impairment called Broca (expressive) aphasia.
If the front part of the frontal lobe is damaged, any of the following may result:
Difficulty temporarily holding information available for processing (called working memory)
Reduced fluency of speech
Apathy (lack of emotion, interest, and concern)
Inattentiveness
Delayed responses to questions
A striking lack of inhibition, including socially inappropriate behavior
People who lose their inhibitions may be inappropriately elated (euphoric) or depressed, excessively argumentative or passive, and vulgar. They may show no regard for the consequences of their behavior. They may also repeat what they say. Some people develop similar symptoms when they get older or if dementia develops. These symptoms may result from degeneration of the frontal lobe.
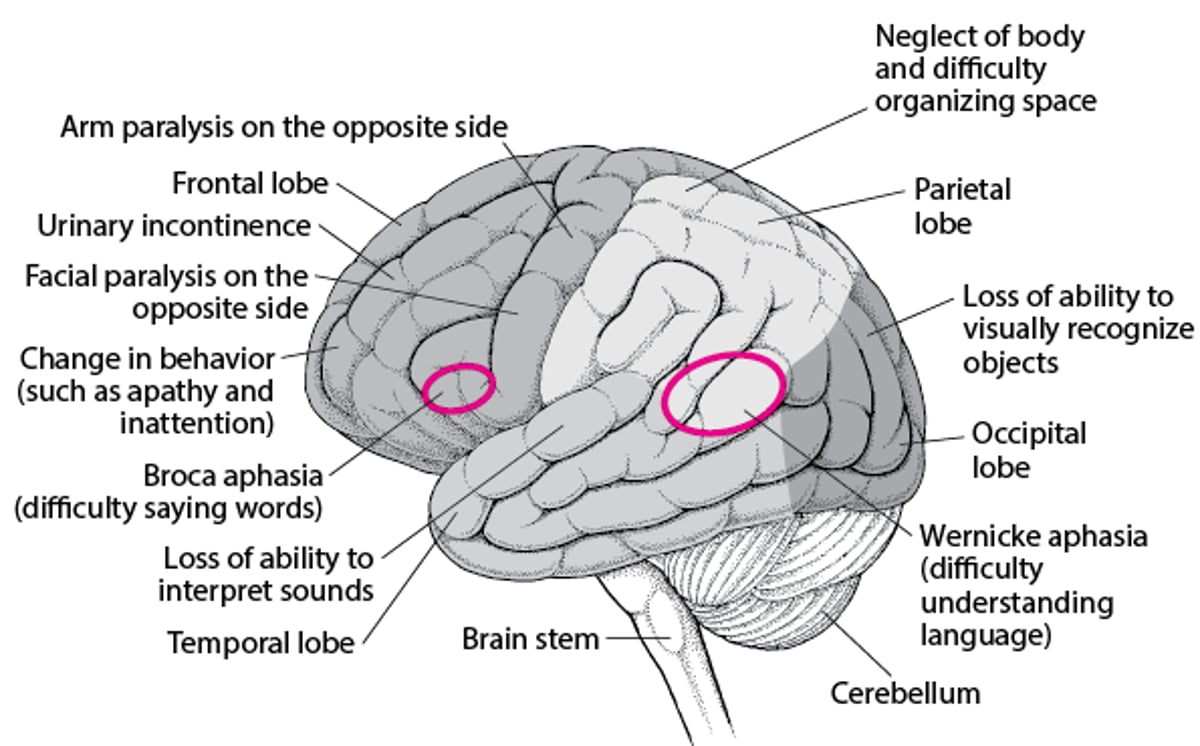
When Specific Areas of the Brain Are Damaged
Different areas of the brain control specific functions. Consequently, where the brain is damaged determines which function is lost. |

Parietal Lobe Damage
The parietal lobes have the following functions:
Interpreting sensory information from the rest of the body
Combining impressions of form, texture, and weight into general perceptions
Influencing mathematical skills and language comprehension
Storing spatial memories that enable people to orient themselves in space (know where they are) and to maintain a sense of direction (know where they are going)
Processing information that helps people know the position of their body parts
Certain functions tend to be controlled more by one of the parietal lobes (usually the left). It is considered the dominant lobe when it controls language. The other lobe (nondominant) has other functions, such as enabling people to be aware of how the body relates to the space around it.
Damage to the front part of the parietal lobe on one side causes numbness and impairs sensation on the opposite side of the body. Affected people have difficulty identifying a sensation’s location and type (pain, heat, cold, or vibration). People may have difficulty recognizing objects by touch (that is, by their texture and shape).
If the middle part is damaged, people cannot tell the right from the left side (called right-left disorientation) and have problems with calculations and writing. They may have problems sensing where parts of their body are (a sense called proprioception).
If the nondominant (usually right) parietal lobe is damaged, people may be unable to do simple skilled tasks, such as combing their hair or dressing—called apraxia. They may also have trouble understanding how objects relate to each other in space. As a result, they may have trouble drawing and constructing things, and they may get lost in their own neighborhood. These people may also ignore the serious nature of their disorder or deny its existence. They may neglect the side of the body opposite the brain damage (usually the left side).
Temporal Lobe Damage
The temporal lobes have the following functions:
Generating memory and emotions
Processing immediate events into recent and long-term memory
Storing and retrieving long-term memories
Comprehending sounds and images, enabling people to recognize other people and objects and to integrate hearing and speech
In most people, part of the left temporal lobe controls language comprehension. If that part is damaged, memory for words can be drastically impaired, as can the ability to understand language—an impairment called Wernicke (receptive) aphasia (see table Testing a Person With Aphasia).
If certain areas of the right temporal lobe are damaged, memory for sounds and music may be impaired. As a result, people may have trouble singing.
Occipital Lobe Damage
The occipital lobe contains the main center for processing visual information.
The occipital lobes have the following functions:
Processing and interpreting vision
Enabling people to form visual memories
Integrating visual perceptions with the spatial information provided by the adjacent parietal lobes
If both sides of the occipital lobe are damaged, people cannot recognize objects by sight, even though the eyes themselves are functioning normally. This disorder is called cortical blindness. Some people with cortical blindness are unaware that they cannot see. Instead, they often make up descriptions of what they see (called confabulation). This disorder is called Anton syndrome.
Seizures that involve the occipital lobe can cause hallucinations involving vision. For example, people may see lines of color when they look in a certain direction.
Limbic Lobe Damage
The limbic lobe includes structures located deep within the cerebrum and some parts of the adjacent lobes, such as the temporal lobe. These structures have the following functions:
Receiving and integrating information from many areas of the brain, enabling people to experience and express emotions
Helping form and retrieve memories
Helping people connect memories to the emotions experienced when the memories form
Damage that affects the limbic lobe usually results in a variety of problems.
Seizures that result from damage to the temporal lobe area in the limbic lobe usually last only a few minutes. At first, people may not be able to control their feelings or to think clearly. Or they may smell bad odors that are not there (a type of hallucination). They may appear dazed and unaware of their surroundings and make automatic movements, such as repeatedly swallowing or smacking their lips. During the seizure, some people have personality changes such as humorlessness, extreme religiosity, and obsessiveness. People may also have an overwhelming urge to write.
Other Locations
Many functions of the brain are performed by several areas of the brain working together (networks), not by a single area in the brain. Damage to these networks can cause the following:
Agnosia (loss of the ability to identify objects using one or more of the senses)
Amnesia (total or partial loss of the ability to recall experiences or events)
Aphasia (partial or complete loss of the ability to express or understand spoken or written language)
Apraxia (loss of the ability to do tasks that require remembering patterns or sequences of movements)
Dysarthria (loss of the ability to articulate words normally) may be caused by damage to areas of the brain or cranial nerves that control the muscles involved in producing speech or by damage to the nerve fibers that connect these areas.






