


Meningitis is inflammation of the layers of tissue that cover the brain and spinal cord (meninges) and of the fluid-filled space between the meninges (subarachnoid space).
Meningitis can be caused by bacteria, viruses, or fungi, by disorders that are not infections, or by drugs.
Meningitis symptoms include fever, headache, and a stiff neck that makes lowering the chin to chest difficult or impossible, although infants may not have a stiff neck and symptoms may differ in the very old and in people who take drugs that suppress the immune system.
A spinal tap is done to obtain a sample of cerebrospinal fluid for analysis.
Treatment of meningitis depends on the cause (for example, antibiotics for bacterial meningitis) and includes drugs to relieve symptoms.
(See also Overview of Brain Infections and Meningitis in Children.)
The brain and spinal cord are covered by three layers of tissue called meninges. These layers are the
Dura mater (outermost)
Arachnoid membrane (middle)
Pia mater (innermost)
Tissues Covering the Brain
Within the skull, the brain is covered by three layers of tissue called the meninges. |

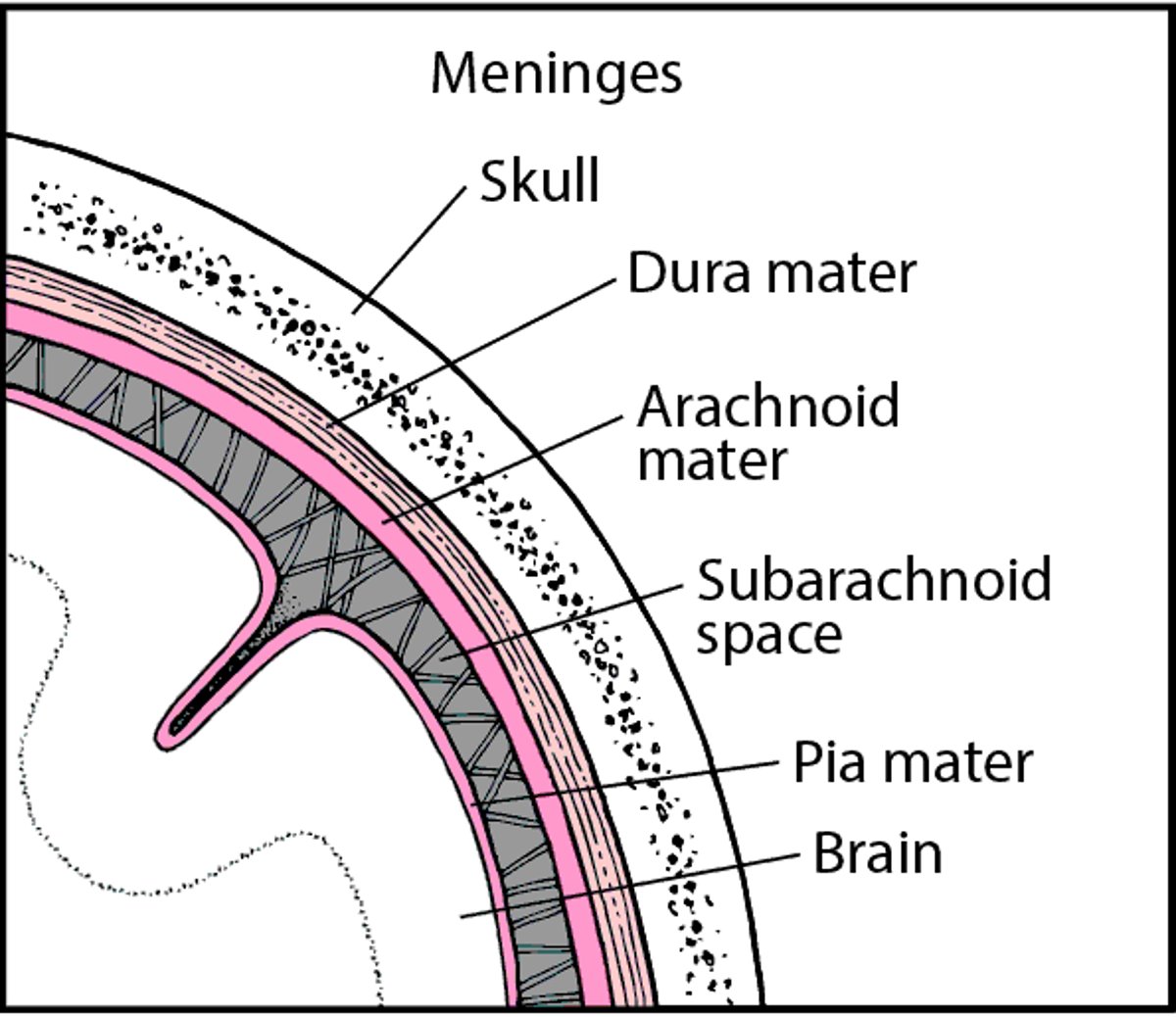
Between the arachnoid membrane and pia mater is the subarachnoid space. This space contains cerebrospinal fluid, which flows through the meninges, fills the spaces within the brain, and helps cushion the brain and spinal cord.
Most often, meningitis is caused by
Infection with microorganisms such as bacteria, viruses, or fungi
However, certain drugs and disorders that are not infections occasionally cause meningitis (called noninfectious meningitis). These disorders include the following:
Cancers that have spread to the meninges, including leukemia and lymphoma
Inflammation of the meninges as a reaction to certain drugs, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and drugs that suppress the immune system (immunosuppressants)
Meningitis often appears suddenly (called acute meningitis). Sometimes it develops over a period of several days to a few weeks (called subacute meningitis). If it lasts 4 weeks or longer, it is considered chronic. It can recur after it has seemed to disappear (called recurrent meningitis).
Meningitis can be classified by what causes it (bacteria, viruses, or something else) or by how quickly it develops (acute, subacute, or chronic). But it is usually classified as one of the following:
Acute bacterial meningitis (which is the most immediately dangerous type)
Noninfectious meningitis (due to disorders that are not infectious or due to drugs or vaccines)
Acute bacterial meningitis is particularly serious and worsens rapidly. Most people with viral or noninfectious meningitis recover within a few weeks. Subacute meningitis and chronic meningitis usually progress slowly and gradually, but doctors may have difficulty determining what the cause is and thus what the treatment should be.
Aseptic meningitis, often used to refer to viral meningitis, actually refers to meningitis caused by anything other than the bacteria that usually cause acute bacterial meningitis. Thus, aseptic meningitis can include meningitis caused by the following:
Viruses
Occasionally, other organisms (such as the bacteria that cause Lyme disease or syphilis)
Disorders that are not infections (such as sarcoidosis)
Reactions to drugs
Symptoms of Meningitis
Different types of meningitis may cause different symptoms. Also, symptoms differ in how severe they are and how quickly they develop. However, all types cause the following:
A painful, stiff neck that makes lowering the chin to the chest difficult or impossible
Headache
Fever
However, these symptoms are often absent or not easily identified in infants. Also, a stiff neck or fever may be absent in the very old or in people who are taking drugs or have conditions that suppress the immune system (immunosuppressants).
People may also appear sluggish or unresponsive.
Diagnosis of Meningitis
Spinal tap and analysis of cerebrospinal fluid
Doctors often suspect meningitis based on symptoms. But because meningitis can be serious, tests are done.
If doctors suspect bacterial meningitis, they first take a sample of blood to test and culture (to grow microorganisms) to determine whether bacteria are present, and, if so, to identify them. However, bacterial meningitis cannot be diagnosed by blood tests.
For all types of meningitis, doctors do a spinal tap (lumbar puncture) to confirm the diagnosis and identify the cause. The sample of cerebrospinal fluid is withdrawn and sent to a laboratory to be examined, analyzed, and cultured.
During a spinal tap, a thin needle is inserted between two bones (vertebrae) in the lower spine to withdraw cerebrospinal fluid.
Then the following are done:
Close examination of the cerebrospinal fluid: The fluid is normally clear but may be cloudy in people with meningitis.
Measurement of the pressure in the subarachnoid space (which contains the cerebrospinal fluid) before the cerebrospinal fluid is withdrawn: Pressure is usually high in meningitis.
Analysis of cerebrospinal fluid in a laboratory: Sugar and protein levels and the number and type of white blood cells in the fluid are determined. This information helps doctors diagnose meningitis and distinguish between bacterial and viral meningitis.
Examination of cerebrospinal fluid under a microscope to check for and identify bacteria. A special stain (called Gram stain) is used to show the bacteria more clearly and to help identify them.
Other tests
However, if they suspect that pressure within the skull is greatly increased (for example, by an abscess, tumor, or another mass in the brain), computed tomography (CT) or magnetic resonance imaging (MRI) may be done first to check for such masses. Doing a spinal tap when pressure within the skull is increased may be dangerous. Parts of the brain may shift downward. If these parts are pressed through the small openings in the tissues that separate the brain into compartments, a life-threatening disorder called brain herniation results.
If a spinal tap cannot be done right away and doctors suspect bacterial meningitis, doctors begin treatment with antibiotics without waiting for test results. After pressure within the skull is lowered or if no mass is detected, a spinal tap is done, and doctors adjust treatment, if needed, after they get the results.
Treatment of Meningitis
For meningitis due to an infection, antimicrobial drugs
General measures and drugs to relieve symptoms
Treatment of meningitis depends on the cause. If meningitis is caused by an infection, appropriate antimicrobial drugs (such as antibiotics, antiviral drugs, or antifungal drugs) are used.
If doctors suspect that meningitis is caused by bacteria or if people appear very ill, they treat the person with antibiotics immediately—without waiting for test results—because bacterial meningitis progresses rapidly and is life threatening. People may also be given corticosteroids to reduce swelling in the brain.
General measures may help relieve symptoms when meningitis is caused by conditions such as a viral infection or a reaction to a drug. When meningitis is mild, drinking plenty of fluids, resting, and taking over-the-counter (OTC) drugs can help relieve fever and pain.
If meningitis is severe, people are admitted to the hospital for treatment.






