


Acute bacterial meningitis is rapidly developing inflammation of the layers of tissue that cover the brain and spinal cord (meninges) and of the fluid-filled space between the meninges (subarachnoid space) when it is caused by bacteria.
Older children and adults develop a stiff neck that makes lowering the chin to the chest difficult or impossible, usually with a fever and headache.
Infants may not develop a stiff neck but may seem generally unwell and have a high or low body temperature, feed poorly, or be irritable or drowsy.
Bacterial meningitis is a medical emergency and is treated as soon as possible, before the diagnosis is confirmed.
To diagnose meningitis, doctors do a spinal tap (lumbar puncture) as soon as possible.
Vaccines can prevent some types of bacterial meningitis.
(See also Introduction to Meningitis.)
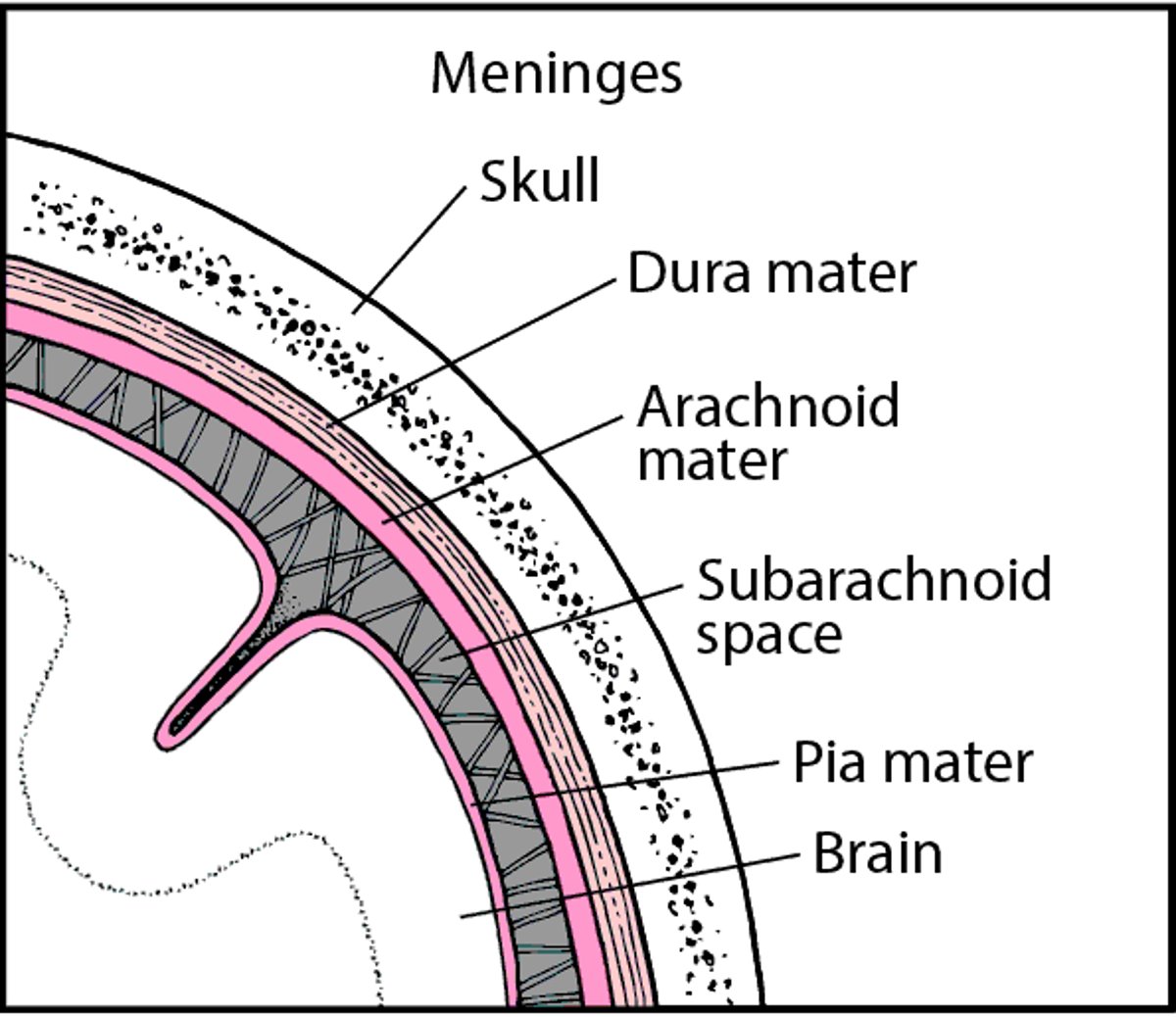
The brain and spinal cord are covered by three layers of tissue called meninges. The subarachnoid space is located between the middle layer and the inner layer of the meninges, which cover the brain and spinal cord. This space contains the cerebrospinal fluid, which flows through the meninges, fills the spaces within the brain, and helps cushion the brain and spinal cord.
Tissues Covering the Brain
Within the skull, the brain is covered by three layers of tissue called the meninges. |

Complications
When bacteria invade the meninges and subarachnoid space, the immune system eventually reacts to the invaders, and immune cells gather to defend the body against them. The result is inflammation—meningitis—which can cause complications such as the following:
Blood clots: If severe, inflammation may spread to blood vessels in the brain and cause clots to form, sometimes resulting in a stroke.
Swelling in the brain (cerebral edema): Inflammation can damage brain tissue, causing swelling and small areas of bleeding.
Increased pressure within the skull (intracranial pressure): Severe swelling can increase pressure within the skull, causing parts of the brain to shift. If these parts are pressed through the small openings in the tissues that separate the brain into compartments, a life-threatening disorder called brain herniation results.
Excess fluid in the brain: The brain continuously produces cerebrospinal fluid. Infection may block it from flowing through the spaces within the brain (ventricles) and out of the brain. Fluid may accumulate in the ventricles, causing them to enlarge (a disorder called hydrocephalus). As excess fluid accumulates, it can put pressure on the brain.
Inflammation of cranial nerves: Inflammation may spread to the cranial nerves, which are involved in sight, hearing, taste, and control of facial muscles and glands. Inflammation of these nerves may result in deafness, double vision, and other problems.
Subdural empyema: Sometimes pus collects under the outer layer (dura mater) of the meninges, causing a subdural empyema.
Bodywide problems: These problems include septic shock (dangerously low blood pressure due to bacterial infection of the bloodstream) and disseminated intravascular coagulation (development of small blood clots throughout the bloodstream, eventually leading to excessive bleeding). These problems can be fatal.
Causes of Acute Bacterial Meningitis
Different species of bacteria can cause meningitis. The bacteria most likely to be the cause depends on
How old people are
How they acquired meningitis (the route)
How strong their immune system is
Age
Acute bacterial meningitis can develop in infants and children, particularly in geographic areas where children are not vaccinated. As people age, acute bacterial meningitis becomes more common.
In newborns and young infants, the most common causes of bacterial meningitis are
Group B streptococci, particularly Streptococcus agalactiae
Escherichia (E.) coli and related bacteria (called gram-negative bacteria)
Listeria monocytogenes
If meningitis develops within the first 48 hours after birth, it is usually acquired from the mother. It may be transmitted from mother to newborn as the newborn passes through the birth canal. In these cases, meningitis is often part of a serious bloodstream infection (sepsis).
In older infants, children, and young adults, the most common causes are
Neisseria meningitidis (also called meningococci)
Streptococcus pneumoniae (also called pneumococci)
Neisseria meningitidis occasionally causes a rapid, severe infection called meningococcal meningitis, resulting in coma and death within hours. This infection commonly occurs when bacteria from an upper respiratory infection enter the bloodstream. Meningococcal meningitis is highly contagious. Small epidemics of meningococcal meningitis may occur among people living in close quarters, as occurs in military barracks and college dormitories. Neisseria meningitidis becomes less common as people age.
Haemophilus influenzae type B is now a rare cause of meningitis in the United States and Western Europe because most children are vaccinated against this bacteria. However, in areas where the vaccine is not widely used, these bacteria are a common cause, particularly in children aged 2 months to 6 years.
In middle-aged and older adults, the most common cause is
Streptococcus pneumoniae
As people age, the immune system weakens, increasing their risk of meningitis due to other bacteria, such as Listeria monocytogenes, E. coli, or other gram-negative bacteria.
In people of all ages, Staphylococcus aureus occasionally causes severe meningitis.
Route of entry
Bacterial meningitis can be acquired in different ways, including
When the bacteria spread through the bloodstream from an infection in another part of the body (the most common route)
When bacteria spread to the meninges from another infection in the head, such as sinusitis or an ear infection (often caused by Streptococcus pneumoniae)
After a wound penetrates the skull or meninges (often caused by Staphylococcus aureus)
When surgery is done on the brain or spinal cord (often caused by gram-negative bacteria)
When a drain (shunt), placed in the brain to relieve increased pressure in the skull, becomes infected
When bacteria enter through a birth defect in the skull or spine (such as spina bifida)
Having any of the above conditions increases the risk of developing bacterial meningitis.
Strength of the immune system
Which bacteria are likely to cause meningitis depends on whether the immune system is normal or weakened. Conditions that can weaken the immune system increase the risk of developing bacterial meningitis. Such conditions include
Treatment with corticosteroids or other drugs that suppress the immune system (immunosuppressants), which are used to treat autoimmune disorders and cancer or to prevent rejection of a transplanted organ
Chemotherapy
Removal of the spleen (splenectomy)
Congenital immunodeficiency disorders (when children are born with a disorder that weakens the immune system)
Which bacteria (or fungi) are likely to cause meningitis also depends on what is weakening the immune system and which part of the immune system is weakened, as in the following examples:
AIDS or Hodgkin lymphoma: Listeria monocytogenes, the bacteria that cause tuberculosis, or fungi (particularly Cryptococcus neoformans)
Problems producing antibodies (which help the body fight infection) or removal of the spleen: Streptococcus pneumoniae or, less often, Neisseria meningitidis, which may cause a rapid, severe form of meningitis
Recent chemotherapy for cancer: Pseudomonas aeruginosa or gram-negative bacteria such as E. coli
In very young infants (particularly premature infants) and older people, certain parts of the immune system may be weak, increasing the risk of meningitis due to Listeria monocytogenes.
Symptoms of Acute Bacterial Meningitis
Symptoms of acute bacterial meningitis vary by age.
In newborns and infants, early symptoms usually do not suggest a particular cause. Symptoms most often include
A high or low body temperature
Feeding problems
Vomiting
Irritability, such as excessive fussiness or crying that continues or worsens after being comforted and cuddled by the mother or caregiver
Smacking the lips, chewing involuntarily, gazing in different directions, or periodically going limp (a type of seizure)
Sluggishness or listlessness (lethargy)
A high-pitched crying that is unusual for the baby
Unlike older children and adults, most newborns and infants do not have a stiff neck. If meningitis becomes severe, the soft spots between skull bones (called fontanelles), which are present in infants before their skull bones grow together, may bulge because pressure within the skull is increased.
In most children and adults, acute bacterial meningitis begins with symptoms that slowly worsen for 3 to 5 days. These symptoms may include a general feeling of illness, fever, irritability, and vomiting. Some people have a sore throat, cough, and a runny nose. These vague symptoms may resemble those of a viral infection.
Early symptoms that suggest meningitis specifically include
Fever
Headache
A stiff neck (usually)
Confusion or decreased alertness
Sensitivity to light
The stiff neck due to meningitis is more than just sore. Trying to lower the chin to the chest causes pain and may be impossible. Moving the head in other directions is not as difficult. However, some people do not have a stiff neck, and some have back pain.
Some people have symptoms of a stroke, including paralysis. Some have seizures.
As infection progresses, children and adults can become increasingly irritable, confused, and then drowsy. They may then become unresponsive and require vigorous, physical stimulation to be aroused. This mental state is called stupor.
Adults may become seriously ill within 24 hours, and children even sooner. Meningitis may cause coma and death within hours. Bacterial meningitis is one of the few disorders in which a previously healthy young person may go to sleep with mild symptoms and never awaken. In older children and adults, such a rapid death often results from swelling of the brain.
In meningococcal meningitis, the bloodstream and many other organs are often infected. The bloodstream infection (called meningococcemia) can become severe within hours, and blood clots may form. As a result, areas of tissue may die, and bleeding may occur under the skin, causing a reddish purple rash of tiny dots or larger splotches. Bleeding can occur in the digestive tract and other organs. People may vomit blood, or stool may appear bloody or tarry black. Without treatment, blood pressure drops, leading to shock and death. Typically, bleeding occurs in the adrenal glands, which shut down, making shock worse. This disorder, called Waterhouse-Friderichsen syndrome, is often fatal unless treated promptly.
In some situations, symptoms of bacterial meningitis are much milder than normal, making the disorder more difficult for doctors to recognize. Symptoms are milder when people are being treated with antibiotics for another reason. For example, they may be being treated for another infection (such as an ear or throat infection) when meningitis develops, or early meningitis may be mistaken for another infection and be treated with antibiotics.
Symptoms can also be milder in people with a weakened immune system due to use of drugs or disorders that suppress the immune system (such as AIDS), in people with alcohol use disorder, and in very old people. In the very old, the only symptom may be confusion.
If bacterial meningitis develops after surgery on the brain or spinal cord, symptoms often take days to develop.
Diagnosis of Acute Bacterial Meningitis
Spinal tap and analysis of cerebrospinal fluid
Children require immediate medical attention, usually in an emergency department, if they do any of the following:
Become increasingly irritable or unusually sleepy
Have a low body temperature
Refuse to eat
Have seizures
Develop a stiff neck
Adults require immediate medical attention if they have any of the following:
A headache and a stiff neck especially if they have a fever
Confusion or decreased alertness
Sluggishness or listlessness
Seizures
Rash with a fever or stiff neck
During the physical examination, doctors look for telltale signs of meningitis, particularly a stiff neck. They also look for a rash, especially in children, adolescents, and young adults, and for other symptoms, which may suggest a cause. Doctors may strongly suspect bacterial meningitis based on symptoms and results of the examination, but tests are needed to confirm the diagnosis and to identify the specific bacteria causing it.
As soon as doctors suspect bacterial meningitis, they take a sample of blood to be grown in a laboratory (cultured) and analyzed. Then they start treatment with antibiotics and corticosteroids immediately, without waiting for test results, because meningitis can progress rapidly.
Did You Know...
|
Tests
Once treatment has started, doctors quickly do a spinal tap (lumbar puncture), if it seems safe, to confirm the diagnosis.
However, if they suspect that pressure within the skull is greatly increased (for example, by an abscess, tumor, or another mass in the brain), computed tomography (CT) or magnetic resonance imaging (MRI) may be done first to check for such masses. Doing a spinal tap when pressure within the skull is increased may be dangerous. Parts of the brain may shift downward. If these parts are pressed through the small openings in the tissues that separate the brain into compartments, a life-threatening disorder called brain herniation results. After pressure within the skull is lowered or if no mass is detected, a spinal tap is done, and doctors adjust treatment, if needed, after they get the results.
During a spinal tap, a thin needle is inserted between two bones (vertebrae) in the lower spine to withdraw cerebrospinal fluid.
Then the following are done:
Close examination of the cerebrospinal fluid: The fluid is normally clear but may be cloudy in people with meningitis.
Measurement of the pressure in the subarachnoid space (which contains the cerebrospinal fluid) before the cerebrospinal fluid is withdrawn: Pressure is usually high in meningitis.
Analysis of cerebrospinal fluid in a laboratory: Sugar and protein levels and the number and type of white blood cells in the fluid are determined. This information helps doctors diagnose meningitis and distinguish between bacterial and viral meningitis.
Examination of cerebrospinal fluid under a microscope to check for and identify bacteria. A special stain (called Gram stain) is used to show the bacteria more clearly and to help identify them.
Other tests
Other tests may be used to rapidly identify certain bacteria, such as Neisseria meningitidis and Streptococcus pneumoniae. Some of these tests identify specific bacteria by detecting specific proteins (antigens) on the surface of the bacteria. The polymerase chain reaction (PCR) technique, which produces many copies of a gene, may be used to identify the bacteria’s unique DNA sequence. Some tests can rapidly analyze large stretches of genetic material. These tests can identify otherwise undetectable microorganisms in cerebrospinal fluid. However, these tests are not always available.
The cerebrospinal fluid is also cultured (to make bacteria grow). Culture helps doctors determine whether bacteria are present and, if so, which bacteria are present and which antibiotics may be most effective. Culture results usually take 24 hours or more. If culture or other tests detect bacteria in cerebrospinal fluid, bacterial meningitis is confirmed.
Until the cause of meningitis is confirmed, other tests using samples of cerebrospinal fluid or blood may be done to check for viruses, fungi, cancer cells, and other substances that routine tests do not identify. Testing for herpes simplex virus, which can infect the brain (causing encephalitis), is particularly important.
Doctors also take samples of blood, urine, and mucus from the nose and throat. In people who have a rash, they may use a small needle to remove fluid and tissue from under the skin where the rash is. These samples are cultured and examined under the microscope to see whether bacteria are present.
Prognosis for Acute Bacterial Meningitis
If treated early, most people with meningitis recover well. But when treatment is delayed, permanent brain or nerve damage or death is more likely, especially in very young children and people over 60. Mortality rates are
For children under 19 years: As low as 3% but often higher
For adults < 60 years: About 17%
For adults over 60 years: Up to 37%
For people with meningitis that is due to Staphylococcus aureus and not acquired in a hospital (community-acquired): About 43%
In some people, seizures that result from meningitis require lifelong treatment.
People who have had meningitis may have problems such as permanent mental impairment, problems with memory or concentration, learning disabilities, behavioral problems, paralysis, double vision, and partial or complete loss of hearing.
Prevention of Acute Bacterial Meningitis
People with acute bacterial meningitis (particularly meningococcal meningitis) are usually placed in isolation until the infection is controlled and they can no longer spread the infection, usually for about 24 hours.
Vaccines for several forms of bacterial meningitis are available.
Meningococcal meningitis
A vaccine (meningococcal vaccine) can help prevent meningococcal meningitis.
Meningitis due to Streptococcus pneumoniae
A vaccine that helps protect against this infection (pneumococcal vaccine) is routinely given to children (see figure Vaccinating Infants and Children).
Meningitis due to Haemophilus influenzae
Children are now routinely immunized with Haemophilus influenzae type b vaccine (see figure Vaccinating Infants and Children). In high-resource countries, this vaccine has virtually eliminated what once was the most common cause of meningitis in children.
Prevention after exposure to meningitis
Whether children under 2 years old need preventive antibiotics after exposure at day care to someone with meningitis due to Haemophilus influenzae is unclear.
Preventive antibiotics are usually needed only for meningococcal meningitis and meningitis due to Haemophilus influenzae.
Treatment of Acute Bacterial Meningitis
Antibiotics
Replacement of fluids
Because acute bacterial meningitis can lead to permanent brain or nerve damage or death within hours, treatment is started as soon as possible, without waiting for the results of diagnostic tests and often before a spinal tap is done.
At this point, doctors do not know the specific bacteria involved and thus cannot know which antibiotics are most effective. So they choose antibiotics that are effective against the bacteria most likely to be causing the infection, and they usually use two or more antibiotics that are effective against many bacteria. The antibiotics are given intravenously. Also, because inflammation of the brain (encephalitis) due to a herpesvirus may resemble bacterial meningitis, an antiviral drug that is effective against this virus is often given. Once the infecting organism, usually a specific species of bacteria, is identified and tested, the antibiotics are changed to ones that are most effective against that organism, and any unnecessary antibiotics and antiviral drugs are stopped.
Other infections, which may have caused or be caused by meningitis, also require treatment. The infections include sepsis, pneumonia, and a heart infection called bacterial endocarditis.
Fluids lost because of fever, sweating, vomiting, and poor appetite are replaced, usually given by vein (intravenously).
Because bacterial meningitis often affects many organs and causes serious complications, people are usually admitted to the intensive care unit.
Treatment of complications
Complications may require specific treatment.
Seizures: Medications Used to Treat Seizures are given.
Shock: Additional fluids and sometimes drugs (given intravenously) are given to increase blood pressure and treat shock, as may occur in Waterhouse-Friderichsen syndrome.
Coma: Mechanical ventilation may need to be used.
Dangerously increased pressure within the skull (intracranial hypertension):
Subdural empyema: A surgeon may have to drain the pus to ensure a successful recovery.






