Glossopharyngeal neuralgia consists of recurring attacks of severe pain in the back of the throat, the area near the tonsils, the back of the tongue, part of the ear, and/or the area under the back of the jaw. The pain is due to malfunction of the 9th cranial nerve (glossopharyngeal nerve). The glossopharyngeal nerve helps move the muscles of the throat and carries information from the throat, tonsils, and tongue to the brain.
The cause is often unknown but sometimes is an abnormally positioned artery that puts pressure on (compresses) the glossopharyngeal nerve.
People have brief attacks of excruciating pain, affecting one side of the tongue or throat and sometimes an ear.
Doctors diagnose the disorder based on what the pain is like and whether a local anesthetic applied to the back of the throat eliminates the pain.
(See also Overview of the Cranial Nerves.)
Glossopharyngeal neuralgia, a rare disorder, usually begins after age 40 and occurs more often in men.
The vagus (10th cranial) nerve malfunctions at the same time because the vagus nerve and the glossopharyngeal (9th cranial) nerve exit the skull together. Thus, the problem affecting the glossopharyngeal nerve usually also affects the vagus nerve. The vagus nerve helps control the heartbeat. When the vagus nerve malfunctions, the pulse may be abnormal, and abnormal heart rhythms (arrhythmias) may occur.
Causes of Glossopharyngeal Neuralgia
Often, the cause of glossopharyngeal neuralgia is unknown.
But sometimes glossopharyngeal neuralgia occurs when
An abnormally positioned artery compresses the glossopharyngeal nerve near where the nerve exits the brain stem.
The long, pointed bone at the base of the skull (styloid process) is abnormally long and compresses the nerve.
Rarely, the cause is a tumor in the brain or neck, an abscess, a bulge (aneurysm) in an artery in the neck (carotid artery), or multiple sclerosis.
Symptoms of Glossopharyngeal Neuralgia
In glossopharyngeal neuralgia, attacks are brief and occur intermittently, but they cause excruciating pain. Attacks may be triggered by a particular action, such as chewing, swallowing, talking, yawning, coughing, or sneezing. The pain usually begins at the back of the tongue, back of the throat, or the area near the tonsils. Sometimes pain spreads to the ear or the area at the back of the jaw. The pain may last several seconds to a few minutes and usually affects only one side of the throat and tongue.
If the vagus nerve malfunctions, disturbing the heart rate, people may faint.
Diagnosis of Glossopharyngeal Neuralgia
A doctor's evaluation
A test using a cotton-tipped applicator and an anesthetic
Magnetic resonance imaging
Sometimes computed tomography or x-rays
Glossopharyngeal neuralgia is distinguished from trigeminal neuralgia (which causes similar pain) based on the pain’s location or results of a specific test. For the test, a doctor touches the back of the throat with a cotton-tipped applicator. If pain results, the doctor applies a local anesthetic to the back of the throat. If the anesthetic eliminates the pain, glossopharyngeal neuralgia is likely.
Magnetic resonance imaging (MRI) is done to check for tumors. Computed tomography (CT) may be done or x-rays are taken to determine whether the styloid process is abnormally long.
A local anesthetic may be applied to back of the throat to help with diagnosis and to rule out other possible causes of the pain. Nerve blocks can also help doctors confirm the diagnosis. They can identify the affected nerve because they are used to disrupt a specific nerve pathway that transmits or enhances pain signals.
Treatment of Glossopharyngeal Neuralgia
Antiseizure medications
A local anesthetic
Sometimes surgery
The same medications used to treat trigeminal neuralgia—antiseizure medicationstricyclic antidepressants, taken by mouth, may help. (Antiseizure medications stabilize nerve cell membranes.) A nerve block may be used immediately for pain relief until the medication taken by mouth takes effect.
However, for permanent relief, surgery may be needed. The glossopharyngeal nerve is separated from the artery that is compressing it by placing a small sponge between them (called vascular decompression).
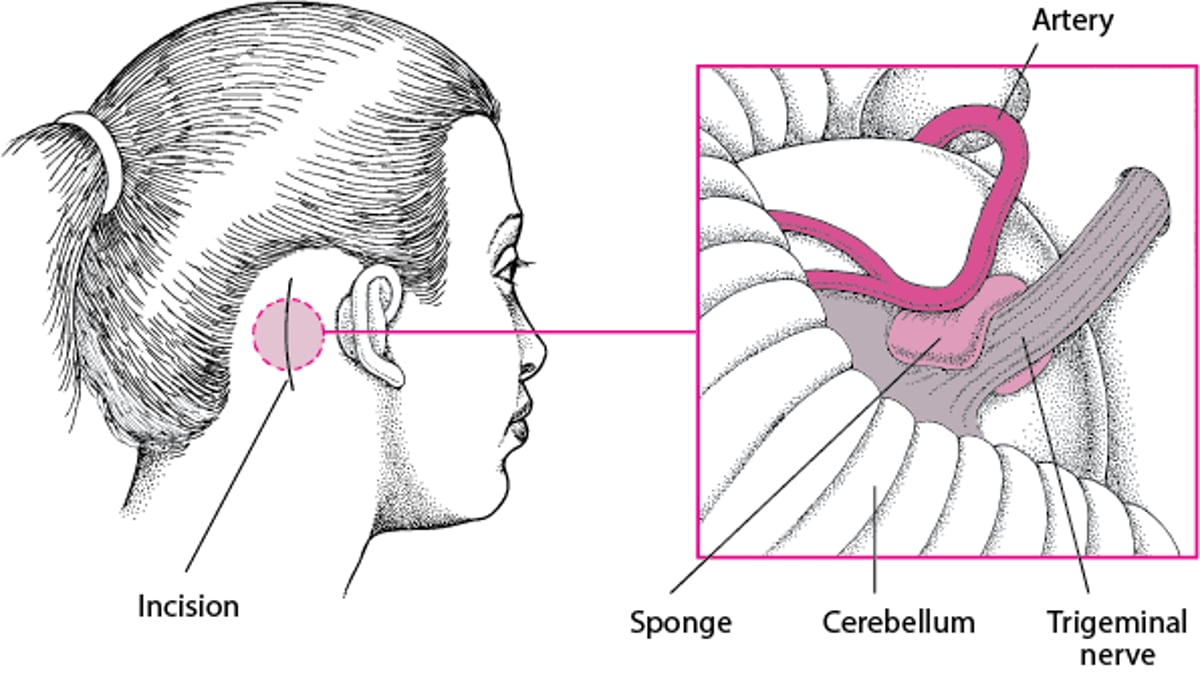
Taking the Pressure Off a Nerve
When pain results from an abnormally positioned artery pressing on a cranial nerve, the pain can be relieved by a surgical procedure called vascular decompression. This procedure may be done to treat trigeminal neuralgia, hemifacial spasms, or glossopharyngeal neuralgia. If the trigeminal nerve is compressed, an area on the back of the head is shaved, and an incision is made. The surgeon cuts a small hole in the skull and lifts the edge of the brain to expose the nerve. Then the surgeon separates the artery from the nerve and places a small sponge between them. A general anesthetic is required, but the risk of side effects from the procedure is small. Side effects include facial numbness, facial weakness, double vision, infection, bleeding, alterations in hearing and balance, and paralysis. Usually, this procedure relieves the pain, but in about 15% of people, pain recurs. |