


Diverticulosis is the presence of one or more balloon-like sacs (diverticula), usually in the large intestine (colon).
The cause of diverticulosis is unknown but may be related to diet, a sedentary lifestyle, obesity, smoking, and use of certain medications.
Spasms of the muscular layer of the intestine are thought to cause diverticula.
Diverticula usually cause no symptoms, but sometimes they become inflamed or bleed, causing blood in the stool or bleeding from the rectum.
Typically, the diagnosis is confirmed by colonoscopy or a computed tomography (CT) scan.
If people have symptoms, a high-fiber diet and stool-bulking agents are given, but sometimes bleeding occurs and requires colonoscopy or even surgery.
What Is Diverticulosis?
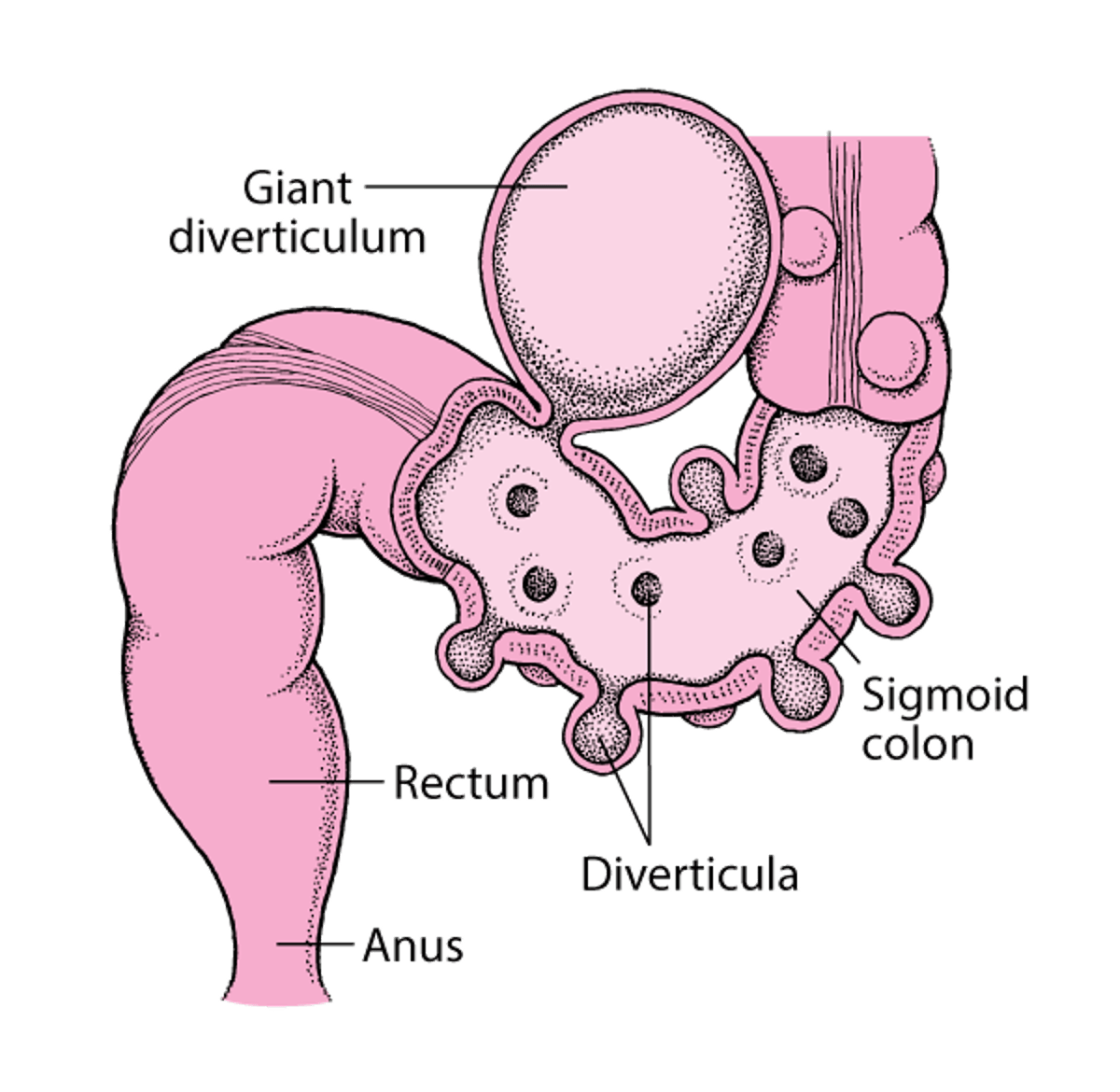
In diverticulosis, many balloon-like sacs (diverticula) develop in the large intestine, most commonly in the last part of it (sigmoid colon). Most diverticula vary in diameter from 1/10 inch to more than 1 inch (about ¼ centimeter to more than 2½ centimeters). For unclear reasons, some diverticula become very large—up to 6 inches (about 15 centimeters) in diameter. |

(See also Definition of Diverticular Disease.)
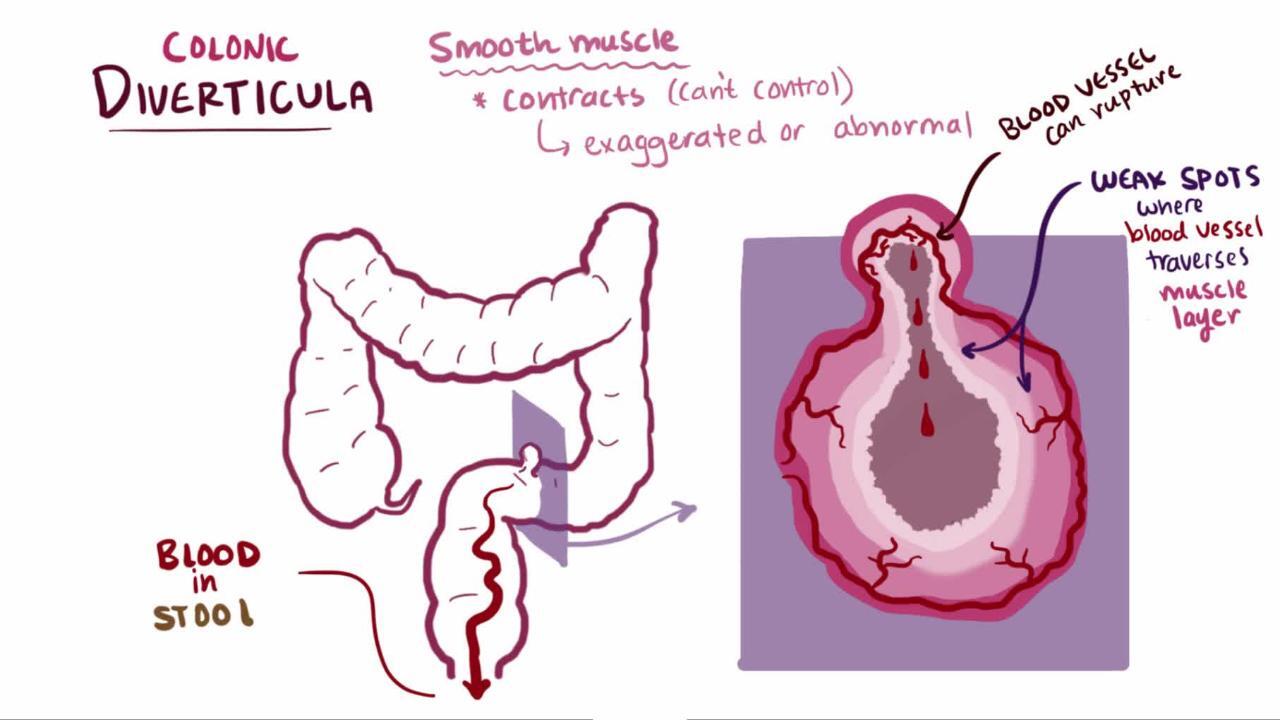
Diverticula in the large intestine occur when a defect develops in the thick, muscular middle layer of the bowel. The thin inner layers of the bowel bulge out through the defect and create a small sac. Diverticula usually do not cause any problems but they sometimes become inflamed or bleed.
Diverticula may develop anywhere in the large intestine, but they are more common in the sigmoid colon, which is the last part of the large intestine just before the rectum. Diverticula vary in diameter from 1/10 inch to almost half an inch (about 3 to more than 10 millimeters). They are uncommon before age 40 but become more common rapidly thereafter. Most people over age 80 have diverticula. Giant diverticula, which are rare, are larger than 1½ inches (about 4 centimeters) in diameter. A person may have only a single giant diverticulum.
Causes of Diverticulosis of the Large Intestine
The cause of diverticulosis is unknown but may be related to a diet low in fiber or high in red meat, a sedentary lifestyle, obesity, and smoking and use of nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, acetaminophen, corticosteroids, and opioids. Other possible risk factors include family history and alterations in the structure of the large intestine and the way in which waste products move through it.
Diverticula are thought to be caused by spasms of the muscular layer of the intestine. The resulting pressure that these spasms exert on the intestinal wall causes a part of the wall to bulge at a point of weakness, usually near to where an artery penetrates the muscular layer of the large intestine. An increase in the thickness of the muscular layer is a common finding in the sigmoid colon of people with diverticulosis.
The cause of a giant diverticulum is unclear.
Symptoms of Diverticulosis of the Large Intestine
Diverticula themselves are not dangerous. In fact, most people with diverticulosis do not have symptoms. However, people with diverticulosis can sometimes have unexplained painful cramps or bowel movement disturbances (such as constipation).
Complications of diverticulosis
Complications of diverticulosis are more common among people who smoke, have obesity, have HIV infection, take NSAIDs, or are undergoing cancer chemotherapy.
The most common complications are
Diverticulitis is inflammation with or without infection of a diverticulum, which causes abdominal pain and can result in a collection of pus (abscess) around the inflamed diverticulum. If a hole (perforation) develops in the diverticulum, fluid and bacteria can leak into the abdomen and cause a very serious condition called peritonitis.
A diverticulum can bleed into the intestine. Bleeding is painless but can be heavy and result in blood passing out through the rectum (see Gastrointestinal Bleeding). Most episodes of bleeding stop spontaneously. However, in some people, doctors have to do colonoscopy or surgery to stop the bleeding. The bleeding may be serious enough to require a blood transfusion.
Diagnosis of Diverticulosis of the Large Intestine
Colonoscopy or computed tomography (CT) scan
Diverticulosis is suspected when symptoms such as unexplained painful cramps, bowel movement disturbances, or painless rectal bleeding, especially in an older person, are present.
Diverticula that do not cause symptoms are usually found incidentally during colonoscopy, colon capsule endoscopy, barium enema, CT scan, or magnetic resonance imaging (MRI).
The diagnosis of diverticulosis is usually confirmed by examining the large intestine using a flexible viewing tube (colonoscopy) or sometimes a CT scan of the abdomen. If the person has severe abdominal pain, doctors usually prefer CT so as not to rupture the inflamed intestine.


If blood is present in the stool, a colonoscopy is usually the best method with which to identify the source. However, in people who are bleeding a lot, CT angiography or radionuclide scans taken after radioactive red blood cells are injected into a vein (intravenously) may be required to determine the source of bleeding.
Treatment of Diverticulosis of the Large Intestine
No treatment for people who have no symptoms
Changes in diet for people who have symptoms
Treatment of bleeding
People who have diverticula but have no symptoms do not need treatment or changes to their diet.
Most bleeding stops without treatment, but, if it does not, doctors often do colonoscopy to locate and clot (coagulate) the bleeding area with clips, heat, or a laser, or by injecting the area with a drug.
Alternatively, doctors may do angiography to stop the bleeding. During this procedure, doctors pass a catheter into the artery that goes to the bleeding diverticulum and then inject material (a process called embolization) to reduce blood flow to the bleeding diverticulum.
Rarely, if bleeding cannot be stopped or recurs often, doctors may do surgery to remove some or all of the large intestine (a procedure called colectomy).
A giant diverticulum may require surgery because it is likely to become infected and rupture.






