Certain gastrointestinal disorders can be life threatening and require emergency treatment. For many people, emergency treatment involves surgery.
Abdominal pain, often severe, usually accompanies gastrointestinal emergencies. If a person has abdominal pain, a doctor must decide whether immediate surgery is needed to both identify and treat the problem or whether surgery can wait until diagnostic test results are available. Emergency surgery of the abdomen is often done when the abdominal pain seems to result from
A ruptured or perforated (punctured) organ, such as the stomach, appendix (see Appendicitis), or intestine
A hernia with too little blood flow
A blockage of blood flow (see Acute Mesenteric Ischemia and Ischemic Colitis)
An abdominal abscess (a pus-filled pocket of infection)
Not all gastrointestinal disorders are treated with surgery (see Ileus).
Gastrointestinal bleeding, which is typically painless, also can be life threatening. Doctors usually do an endoscopy (an examination of internal structures using a flexible viewing tube) to find and treat the source of bleeding. When the source of the bleeding cannot be found or treated, a surgical procedure is sometimes required.
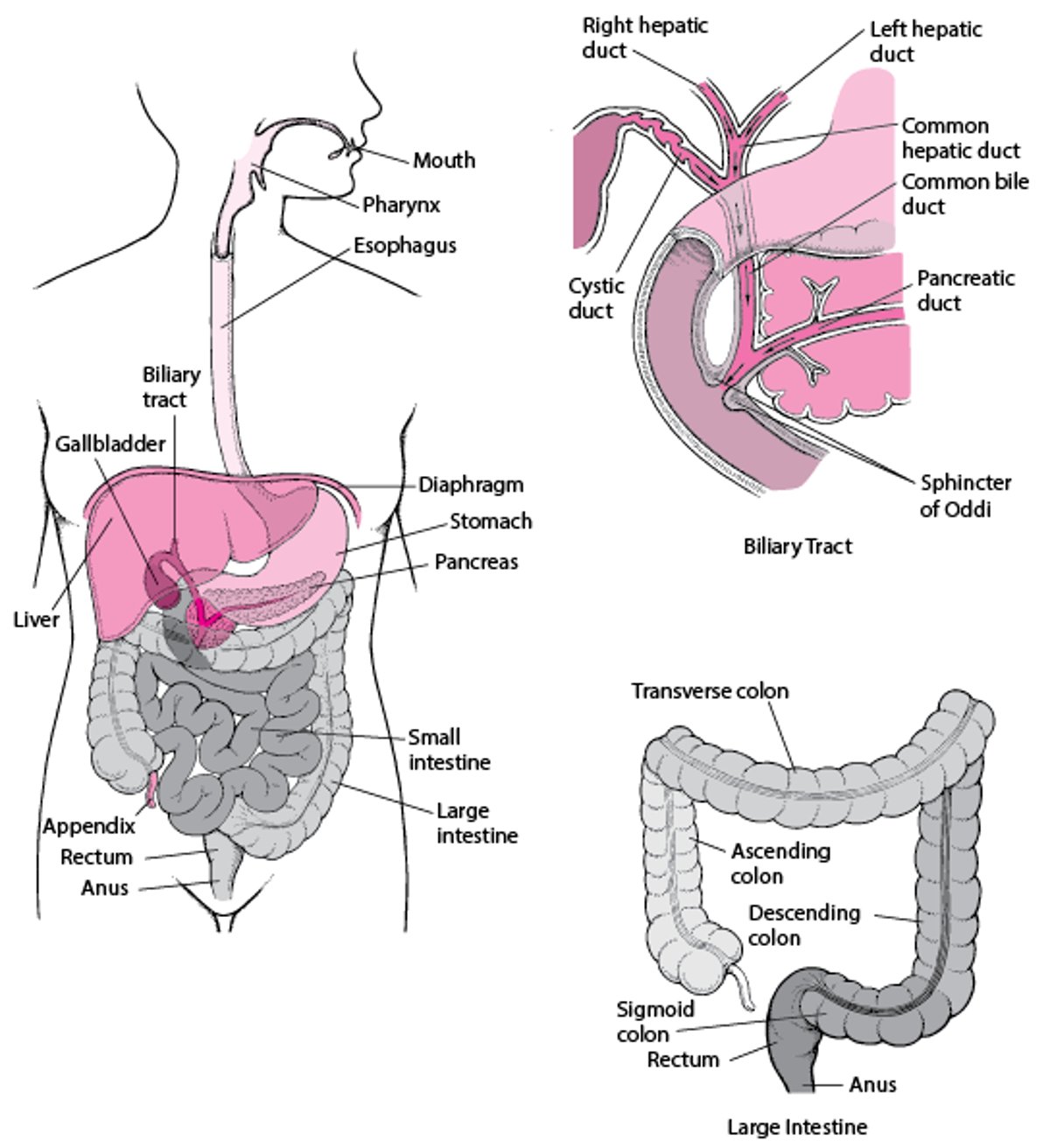
The Digestive System