


Non-Hodgkin lymphomas are a diverse group of cancers of types of white blood cell called lymphocytes.
Often, lymph nodes in the neck, under the arms, or in the groin enlarge rapidly and painlessly.
People may have pain or shortness of breath or other symptoms when enlarged lymph nodes press on organs.
A lymph node and/or bone marrow biopsy are needed for diagnosis.
Treatment may involve radiation therapy, chemotherapy, immunotherapy with monoclonal antibodies, or a combination.
Most people are cured or survive for many years.
People who relapse are treated with stem cell transplantation.
(See also Overview of Lymphoma and Hodgkin Lymphoma.)
Lymphomas are cancers of a specific type of white blood cells known as lymphocytes. These cells help fight infections. Lymphomas can develop from either of the 2 main types of lymphocyte:
B lymphocytes (B cells)
T lymphocytes (T cells)
B lymphocytes produce antibodies, which are essential in fighting off some infections. T lymphocytes are important in regulating the immune system and in fighting viral infections.
Non-Hodgkin lymphomas are actually more than 50 different diseases that involve B cells or T cells. Each of these lymphomas has a distinct appearance under the microscope, a different cell pattern, and a different pattern of symptoms and progression. Most non-Hodgkin lymphomas are from B cells. The remainder develop from T cells.
Non-Hodgkin lymphoma is more common than Hodgkin lymphoma. It is the sixth most common cancer in the United States and causes 4% of all cancer deaths. It is more common as people get older.
In the United States, more than 80,000 new cases are diagnosed every year . People who have had organ transplants and some people who have been infected with hepatitis C virus or the human immunodeficiency virus (HIV) are at risk of developing non-Hodgkin lymphoma.
Leukemias also are cancers that involve white blood cells. In leukemias, most of the cancerous white blood cells are in the bloodstream and bone marrow. In lymphomas, most of the cancerous white blood cells are within lymph nodes and organs such as the spleen and liver. However, leukemia and non-Hodgkin lymphoma sometimes overlap because people with lymphoma may have cancerous white blood cells in their bloodstream and people with leukemia may have cancer cells in their lymph nodes and organs.
Did You Know...
|
Causes of Non-Hodgkin Lymphomas
Although the cause of most non-Hodgkin lymphomas is not known, evidence strongly supports a role for viruses in some of the less common types. The Epstein-Barr virus is associated with Burkitt lymphoma, another type of non-Hodgkin lymphoma. Other suspected viral causes include hepatitis C virus, Kaposi sarcoma herpes virus, and human T-cell lymphotrophic virus type 1 (HTLV-1). People with HIV are at increased risk of developing some subtypes of non-Hodgkin lymphoma. Some bacteria are associated with lymphoma risk, for example, Helicobacter pylori is associated with risk of certain lymphomas in the stomach.
Other people at risk for non-Hodgkin lymphoma include those with
Inherited immunodeficiency syndromes such as ataxia-telangiectasia, Klinefelter syndrome, Chédiak-Higashi syndrome, and Wiskott-Aldrich syndrome
Acquired immunodeficiencies, caused by disorders such as HIV infection or medications used after organ transplantation
A close relative with non-Hodgkin lymphoma
Symptoms of Non-Hodgkin Lymphomas
The first symptom is often rapid and usually painless enlargement of lymph nodes in the neck, under the arms, or in the groin. Enlarged lymph nodes within the chest may press against airways, causing cough and difficulty breathing, or press against blood vessels in the chest, causing swelling of the face, neck, and arms (superior vena cava syndrome). Deep lymph nodes within the abdomen may press against various organs, causing loss of appetite, constipation, abdominal pain, or progressive swelling of the legs.

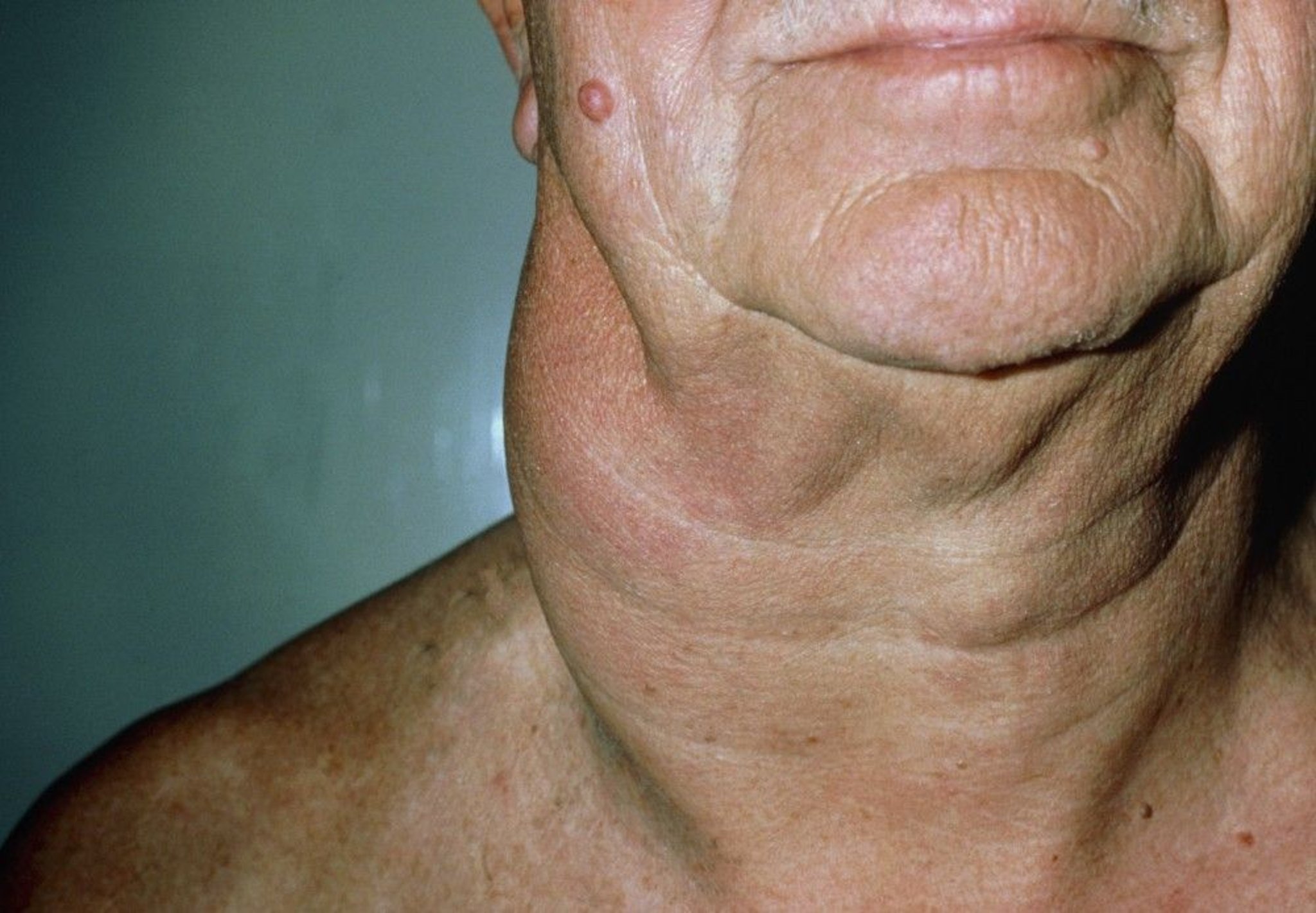
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Some lymphomas can appear in the bloodstream and bone marrow.
Lymphoma cells in the bone marrow may interfere with the ability of the bone marrow to produce enough normal blood cells.
Fever and excessive sweating may indicate infection, which may result from too few normal white blood cells.
Weakness, fatigue, and paleness, which may result from too few red blood cells (anemia). Some people with more severe anemia may have trouble breathing, a rapid heart rate, or chest pain.
Easy bruising and bleeding, sometimes in the form of nosebleeds or bleeding gums, which may result from too few platelets (thrombocytopenia). In some cases, people may bleed into their brain or abdomen.
Non-Hodgkin lymphomas can also invade the digestive tract, skin, and occasionally the nervous system, causing various symptoms. Some people have persistent fever without an evident cause, the so-called fever of unknown origin. This type of fever commonly reflects an advanced stage of disease.
In children, the first symptoms—anemia, rashes, and neurologic symptoms, such as weakness and abnormal sensation—are likely to be caused by infiltration of lymphoma cells into the bone marrow, blood, skin, intestine, brain, and spinal cord. Lymph nodes that become enlarged are usually deep ones, leading to the following:
Accumulation of fluid around the lungs, which causes difficulty in breathing
Pressure on the intestine, which causes loss of appetite or vomiting
Blocked lymph vessels, which causes fluid retention called lymphedema, most noticeably in the arms and legs
Symptoms of Non-Hodgkin Lymphoma
Symptoms | Cause |
|---|---|
Difficulty breathing Swelling of the face | Lymph nodes in the chest are enlarged. |
Loss of appetite Abdominal pain or distention from a blocked bowel or fluid in the abdomen | Lymph nodes in the abdomen are enlarged. |
Lymphoma cells are blocking the flow of bile from the liver. | |
Decreased urine production | Lymph nodes are blocking the flow of urine from the kidney to the bladder |
Progressive swelling of the legs | Lymph vessels in the groin or abdomen are blocked producing lymphedema. |
Weight loss Diarrhea Flatulence Bloating and cramping (indicating malabsorption—nutrients are not absorbed normally into the blood) | Lymphoma cells are growing in or around the small intestine. |
Shortness of breath Chest pain Cough (indicating fluid accumulation around the lungs, called pleural effusion) | Lymph vessels in the chest are blocked. |
Swelling of the face and neck | Blood vessels in the chest are blocked. |
Thickened, dark, itchy areas of skin | Lymphoma cells are infiltrating the skin. |
Weight loss Fever Night sweats | The disease is spreading throughout the body. |
Fatigue Shortness of breath Pale skin (indicating anemia, or too few red blood cells) | One or more of the following occurs:
|
Susceptibility to severe bacterial infections | Lymphoma cells are invading the bone marrow and lymph nodes, reducing antibody production. |
Diagnosis and Classification of Non-Hodgkin Lymphomas
Lymph node biopsy
Doctors suspect non-Hodgkin lymphoma when a person with no apparent infection develops persistent and painless enlargement of lymph nodes that lasts for several weeks. Sometimes enlarged lymph nodes deep within the chest or abdomen are found unexpectedly when a chest x-ray or computed tomography (CT) is done for another reason.
Doctors do a biopsy of an enlarged lymph node to diagnose non-Hodgkin lymphomas and to distinguish them from Hodgkin lymphoma and other disorders that cause enlarged lymph nodes.
The type of biopsy depends on which node is enlarged and how much tissue is needed. Doctors must remove enough tissue to be able to distinguish non-Hodgkin lymphoma from other disorders that can cause lymph node enlargement, including Hodgkin lymphomas, infections, inflammation, or other cancers.
The best way to obtain enough tissue is with an excisional biopsy (a small incision made to remove a piece of the lymph node). Occasionally, when an enlarged lymph node is close to the body's surface, a sufficient amount of tissue can be obtained by inserting a hollow needle (usually under ultrasound or CT guidance) through the skin and into the lymph node (core needle biopsy). When an enlarged lymph node is deep inside the abdomen or chest, surgery may be needed to obtain a piece of tissue.
Although more than 50 different disorders can be called non-Hodgkin lymphomas, doctors sometimes group them into two broad categories.
Indolent lymphomas are characterized by
A long survival period (many years)
Rapid response to many treatments
Variable periods of remission but lack of cure with current standard therapies
Aggressive lymphomas are characterized by
Rapid progression without therapy
High rates of cure with standard chemotherapy but short survival when cure is not achieved
Although non-Hodgkin lymphomas are usually diseases of middle-aged and older adults, children and young adults may develop lymphomas. Lymphomas that develop in children and young adults are commonly aggressive subtypes.
Staging of Non-Hodgkin Lymphomas
Imaging studies
Bone marrow biopsy
Blood tests (including tests of liver and kidney function)
Many people with non-Hodgkin lymphomas have disease that has spread at the time of diagnosis. In only a minority of people, the disease is limited to one region. People with these lymphomas undergo similar staging procedures as people with Hodgkin lymphoma.
Staging is important because the treatment and the prognosis are based on the stage. Several procedures are used to stage or assess non-Hodgkin lymphoma. Basic blood tests, including a complete blood count and tests of liver and kidney function, are done along with tests for infection with human immunodeficiency virus (HIV), hepatitis B virus, and hepatitis C virus.
Positron emission tomography (PET) combined with computed tomography (combined PET-CT) is the most sensitive technique for determining the location and size of cancerous lesions and how active the cancer cells are. If combined PET-CT scan is not available, a contrast CT scan of the chest, abdomen, and pelvis is done. Other tests such as magnetic resonance imaging (MRI) of the brain or spinal cord are done if symptoms of the nervous system are present.
Bone marrow biopsy may be done, particularly when the blood tests show anemia or low platelet counts. In some types of non-Hodgkin lymphoma, the PET-CT scan can reliably detect bone marrow involvement, so a bone marrow biopsy may not always be necessary. In other types of non-Hodgkin lymphoma, the PET-CT scan cannot reliably detect bone marrow involvement and a bone marrow biopsy may be needed if staging would change the choice of treatment.
The disease is classified into 4 stages based on the extent of its spread (I, II, III, IV). The higher the number, the more the lymphoma has spread.
Limited stage disease includes stages I and II. Advanced stage disease includes stages III and IV. In stages I and II, if non-Hodgkin lymphoma is present in an organ outside the lymph system, it is classified as stage IE or IIE. Bulky disease is the term used when there is a tumor mass in the chest, the size of which may be different for different types of lymphomas.
Stages of Non-Hodgkin Lymphoma
Stage | Extent of Spread |
|---|---|
I | Limited to one lymphatic tissue site (lymph node, thymus, or spleen), or only one site outside the lymphatic system (IE)* |
II | Involves two or more lymph node regions on the same side of the diaphragm, above or below it (for example, some enlarged nodes in the neck and some in the armpit), or extension outside an involved lymph node area with or without other lymph node areas on the same side of the diaphragm (IIE)* |
III | Involves spleen and lymph node regions above and below the diaphragm (for example, some enlarged nodes in the neck and some in the groin) |
IV | Involves other parts of the body (such as the bone marrow, lungs, or liver), as well as lymph nodes |
* In stages I and II, if lymphoma is present in an organ outside the lymph system, it is classified as stage IE or IIE. | |
Treatment of Non-Hodgkin Lymphomas
Chemotherapy, radiation therapy, or both
Immunotherapy (drugs made up of antibodies that attack cancer cells), with or without chemotherapy
Sometimes stem cell transplantation
The treatment of non-Hodgkin lymphoma varies widely based on the subtype.
For some people with indolent lymphomas, treatment is not needed when the lymphoma is first diagnosed. Studies show that waiting does not compromise outcome and prevents the person from being exposed to side effects of treatment earlier than necessary. For people with indolent lymphomas, treatment, when needed, extends life and relieves symptoms for many years.
For people with aggressive lymphomas, cure is possible and therefore waiting without treatment is not usually done.
The likelihood of a cure or long-term survival depends on the type of non-Hodgkin lymphoma and the stage when treatment starts. It is somewhat of a paradox that indolent lymphomas usually respond readily to treatment by going into remission (in which the disease is under control), often followed by long-term survival, but the disease usually is not cured. In contrast, aggressive non-Hodgkin lymphomas, which usually require very intensive treatment to achieve remission, have a good chance of being cured.
Stage I non-Hodgkin lymphomas: Limited disease
People with indolent lymphomas who have very limited disease (stage I) are often treated with radiation therapy limited to the site of the lymphoma and adjacent areas. With this approach, most people do not have a disease recurrence in the irradiated area, but non-Hodgkin lymphomas can recur elsewhere in the body as long as 10 years after treatment, so people require long-term monitoring. People with aggressive lymphomas at a very early stage need to be treated with combination chemotherapy and sometimes radiation therapy.
Stage II non-Hodgkin lymphomas: Limited or advanced disease
Stage II non-Hodgkin lymphoma usually behaves like limited disease (stage I) but sometimes behaves like advanced disease. Doctors choose the treatment depending on the disease behavior.
Stages III to IV non-Hodgkin lymphomas: Advanced disease
Almost all people with indolent lymphomas have stage II to IV disease. They do not always require treatment initially, but they are monitored for evidence of lymphoma progression, which could signal a need for therapy, sometimes years after the initial diagnosis. There is no evidence that early treatment extends survival in people with indolent lymphomas at more advanced stages. If the disease begins to progress, there are many treatment choices.
The choice of treatment depends on a variety of factors, including the lymphoma subtype, the extent of spread, the person’s symptoms, and co-existing medical conditions. Treatment may include therapy with monoclonal antibodies (such as rituximab) alone or combined with The choice of treatment depends on a variety of factors, including the lymphoma subtype, the extent of spread, the person’s symptoms, and co-existing medical conditions. Treatment may include therapy with monoclonal antibodies (such as rituximab) alone or combined withchemotherapy. Most treatments are given intravenously. Sometimes, oral medications are used. Treatment usually produces a remission. The average length of remission depends on the intensity of the treatment. Sometimes treatment may also include maintenance therapy (therapy given after the initial treatment to help prevent relapse).
For people with aggressive lymphomas, stage II to IV, combinations of chemotherapy agents are given promptly, often together with rituximab. Many potentially effective combinations of chemotherapy agents are available. Combinations of chemotherapy agents are often given names created by using the initial letter of each drug that is included. For example, one of the oldest and still one of the most commonly used combinations is known as CHOP (cyclophosphamide, [hydroxy]doxorubicin, vincristine [Oncovin], and prednisone). Rituximab has been shown to improve the outcome of CHOP and is now routinely added to the combination (R-CHOP). Other combinations of medications are being studied. agents are given promptly, often together with rituximab. Many potentially effective combinations of chemotherapy agents are available. Combinations of chemotherapy agents are often given names created by using the initial letter of each drug that is included. For example, one of the oldest and still one of the most commonly used combinations is known as CHOP (cyclophosphamide, [hydroxy]doxorubicin, vincristine [Oncovin], and prednisone). Rituximab has been shown to improve the outcome of CHOP and is now routinely added to the combination (R-CHOP). Other combinations of medications are being studied.
Chemotherapy, which often causes different types of blood cells to decrease in number, is sometimes better tolerated if special proteins (called growth factors) are also given to stimulate growth and development of blood cells.
Did You Know...
|
Posttreatment strategies
After radiation therapy, there is an increased risk of secondary cancers occurring 10 or more years after treatment in organs that were in the radiation field. Leukemias may develop in some people many years after successful treatment for non-Hodgkin lymphoma, regardless of the treatment used.
After treatment has been finished, people should have regular doctor's examinations and tests to look for return of the lymphoma (post-treatment surveillance). The type of tests depends on the patient's risk factors and type of treatment they received.
Relapse
Most people who have a relapse of an aggressive lymphoma receive high doses of chemotherapy agents combined with autologous stem cell transplantation, involving the person's own stem cells. With this type of treatment, some people are cured. Sometimes stem cells from a sibling or even an unrelated donor (allogeneic transplant) can be used, but this type of transplantation has a greater risk of complications. Sometimes people are offered treatment with chimeric antigen receptor (CAR) T cells, which are T cells that have been genetically engineered to fight against lymphoma.
More Information
The following English-language resource may be useful. Please note THE MANUAL is not responsible for the content of this resource.
Leukemia & Lymphoma Society: Non-Hodgkin Lymphoma: Comprehensive information on non-Hodgkin lymphomas, including diagnosis, treatment and support







