


Leishmaniasis is caused by 20 or more species of the protozoa Leishmania. Leishmaniasis includes several disorders that affect the skin, the mucous membranes of the nose, mouth, or throat or internal organs including the liver, spleen, and bone marrow.
Leishmania protozoa (single-cell infectious organisms) are usually spread through the bite of infected sand flies.
People may have mild or no symptoms or have skin sores (cutaneous leishmaniasis), or sores in the nose, mouth, or throat that can lead to severe disfigurement (mucosal leishmaniasis), or have fever, weight loss, fatigue, and enlargement of the spleen and liver (visceral leishmaniasis).
Doctors diagnose the infection by analyzing samples of infected tissue or doing blood tests.
Medications used to treat the infection depend on the clinical form of leishmaniasis, the status of the person's immune system, which species of Leishmania is causing the infection, and where the infection was acquired.
Using insect repellents and bed nets and clothing treated with insecticides helps prevent sand fly bites.
(See also Overview of Parasitic Infections.)
Leishmaniasis occurs in scattered areas throughout the world.
Transmission of leishmaniasis
Tiny infected sand flies spread Leishmania when they bite people or animals, such as dogs or rodents. Rarely, infection is spread in blood transfusions, through injection with a needle previously used by an infected person, from mother to child before or at birth, or, very rarely, through sexual contact or laboratory needle-stick accidents.

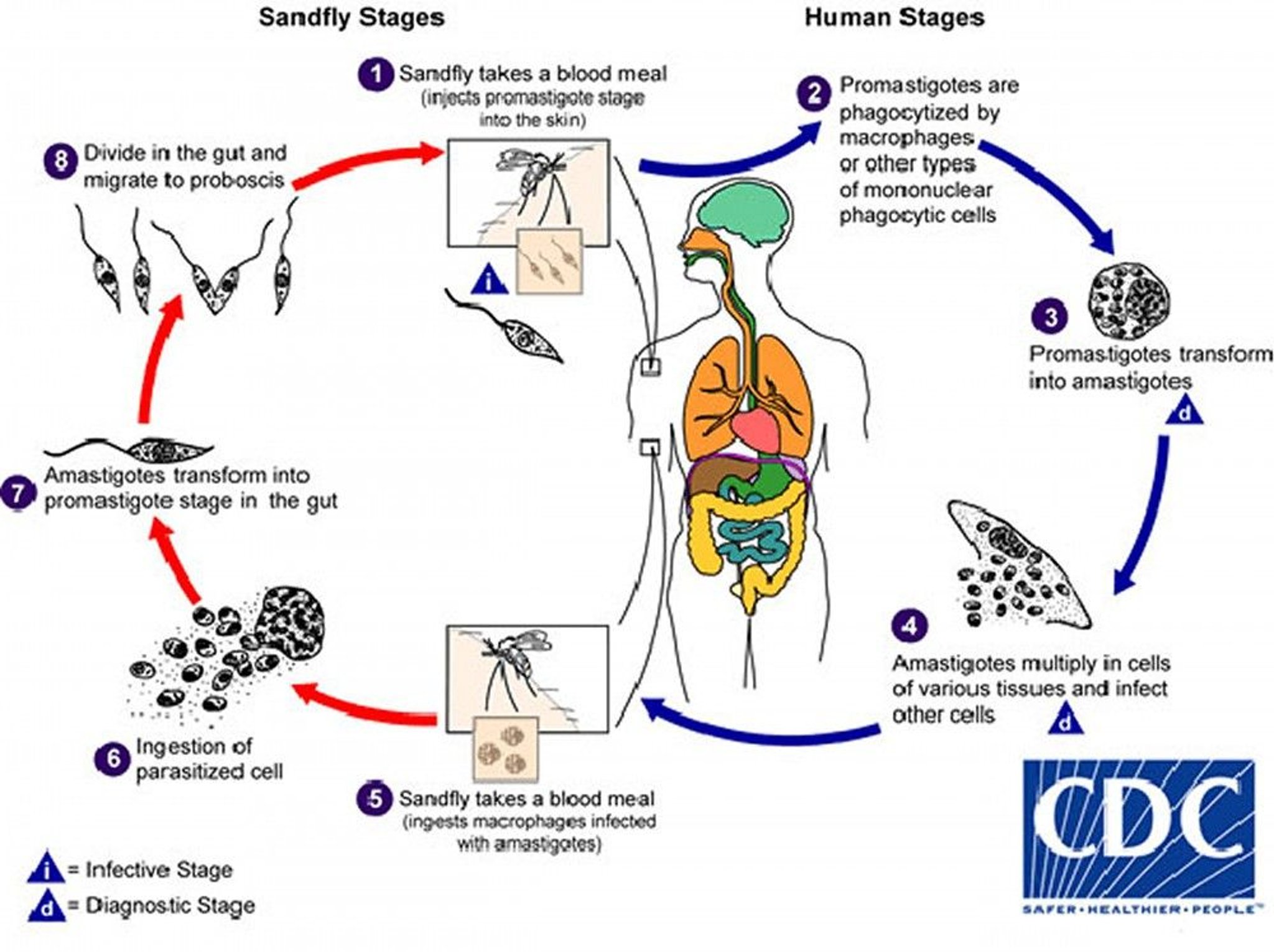
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Clinical forms of leishmaniasis
Leishmaniasis produces a spectrum of disease. There are three major forms. Each affects a different part of the body. After the protozoa enter the body through a bite in the skin, they may remain in the skin or spread to the mucous membranes of the nose, mouth, and throat, or to internal organs including the bone marrow, liver, and spleen.
Cutaneous leishmaniasis affects the skin. It occurs in southern Europe, Asia, Africa, Mexico, and Central and South America. Outbreaks of leishmaniasis have occurred among US military personnel training in Panama or serving in Iraq or Afghanistan. Occasionally, travelers to affected areas develop the disorder.
Mucosal leishmaniasis affects the mucous membranes of the nose and mouth, causing sores and destroying tissue. This form begins with a skin sore. The parasites spread from the skin through the lymph and blood vessels to the mucous membranes. Symptoms of mucosal leishmaniasis can develop while the skin sore is present or months to years after the sore heals.
Visceral leishmaniasis (kala-azar) affects the internal organs, particularly the bone marrow, lymph nodes, liver, and spleen. It occurs in India, Africa (particularly the Sudan and Kenya), Central Asia, the area around the Mediterranean, South and Central America, and rarely China. Parasites spread from the skin to the lymph nodes, spleen, liver, and bone marrow. Not all infected people develop symptoms. Children are more likely to have symptoms than adults in many areas, and the disease is more likely to progress in people with a weakened immune system, particularly those with AIDS, than in people with a healthy immune system.
Symptoms of Leishmaniasis
In cutaneous leishmaniasis, the first symptom is usually a well-defined bump at the site of a sand fly bite. It typically appears after several weeks or months and contains parasites inside white blood cells known as macrophages. As the infection spreads, more bumps may appear near the initial bump. The initial bump slowly enlarges and often becomes an open sore, which may ooze or form a scab. The sores are usually painless and cause no other symptoms unless a secondary bacterial infection, characterised by redness in adjacent areas of the skin, pain, and sometimes fever, develops in them. The sores eventually heal on their own after several months but may persist for more than a year. They leave permanent scars similar to those due to burns. Rarely, sores appear on skin all over the body. When this happens, the person is evaluated for HIV infection and other causes of a weakened immune system.


© Springer Science+Business Media
In mucosal leishmaniasis, symptoms begin with a skin sore that heals on it own. Sores and tissue destruction may appear on mucous membranes inside the nose, mouth, or throat while the skin sore is present or months to years after it heals. The first sign may be a stuffy nose, a discharge from the nose, or nosebleeds. Over time, people may be severely disfigured.


Image courtesy of Dr. A. Canese via the Public Health Image Library of the Centers for Disease Control and Prevention.
Visceral leishmaniasis may start suddenly but usually develops gradually over weeks to months after the infecting sand fly bite. People may have irregular bouts of fever. They may lose weight, have diarrhea, and be generally tired. The liver, spleen, and sometimes lymph nodes enlarge. The number of blood cells decreases, causing anemia and making people more susceptible to other infections. Without treatment, visceral leishmaniasis can result in death.
People who respond to treatment and those who are infected but do not have symptoms are unlikely to have symptoms later unless their immune system is weakened (for example, by AIDS or by medications that are used to suppress the immune system, such as those used to prevent rejection of a transplanted organ).
After treatment of visceral leishmaniasis, patches or lumps (nodules) may appear on the skin as other symptoms of visceral leishmaniasis go away. When sand flies bite people who have these areas of abnormal skin, the flies become infected and can thus spread the infection. Whether patches and lumps appear after treatment and how long they last depend on the geographic location where people were infected:
The Sudan (located south of the Sahara) in Africa: The patches and lumps typically remain a few months to a year.
India and nearby countries: The patches and lumps can last years.
Southern Europe, North Africa, the Middle East, and Latin America: Patches and lumps do not appear on the skin after treatment of visceral leishmaniasis.
In people with AIDS, visceral leishmaniasis often recurs, and cutaneous leishmaniasis can cause sores all over the body.
Diagnosis of Leishmaniasis
Microscopic examination and culture for leishmania and tests for their genetic material (DNA) in samples of infected tissue
Blood tests for visceral leishmaniasis
Doctors diagnose leishmaniasis by taking samples of the infected tissue in people who have skin sores and may have cutaneous leishmaniasis or by taking samples of blood, bone marrow, liver, or spleen in people who may have visceral leishmaniasis. Microscopic examination, culture, and tests to check for the genetic material (DNA) of Leishmania are done to determine whether the samples contain Leishmania.
Blood tests to detect antibodies against Leishmania can sometimes help doctors diagnose visceral leishmaniasis. (Antibodies are proteins produced by the immune system to help defend the body against attack, including that by parasites.) However, results of antibody tests may be negative, particularly in people with a weakened immune system, such as those with AIDS. Blood tests for antibodies are not helpful in diagnosing cutaneous leishmaniasis.
Treatment of Leishmaniasis
Various medications, depending on several factors
If mucosal leishmaniasis causes disfigurement, reconstructive surgery after successful drug therapy
Consultation with an expert on the treatment of leishmaniasis is recommended. Doctors consider the following factors when selecting a medication to treat leishmaniasis:
The form of the disease, whether it is cutaneous, mucosal, or visceral
The Leishmania species responsible
The geographic location where the person was infected
The likelihood that the Leishmania species is susceptible to treatment
The status of the person's immune system
The route of drug administration and the potential side effects
Medications used to treat leishmaniasis include:
liposomal amphotericin B.
miltefosine must use effective birth control measures.
Cutaneous leishmaniasis
For small, uncomplicated sores due to Leishmania species that do not cause mucosal leishmaniasis, treatment options include:
Cryotherapy (freezing) or heat therapy applied to sores
An antileishmanial medication
Leishmania species that is not associated with mucosal leishmaniasis. If it continues to heal, no treatment is needed.
Treatment with an antileishmanial medication is used
For large, multiple, or potentially disfiguring sores
When topical therapy is not available or fails
For sores due to Leishmania braziliensis or related species in Latin America that cause mucosal leishmaniasis
In people with a weakened immune system
When a leishmania skin sore becomes secondarily infected with bacteria, an antibiotic effective for the treatment of skin and soft tissue infections is used.
Mucosal leishmaniasis
The medications of choice are
Reconstructive surgery may be needed if the nose or face is disfigured, but surgery should be delayed for 12 months after treatment to avoid losing a skin graft should a relapse occur.
Visceral leishmaniasis
The medications of choice are
Supportive measures, such as adequate nutrition, blood transfusions, or antibiotics to treat concurrent bacterial infections, may be needed along with antileishmanial therapy.
For people with AIDS
AIDSantiretroviral medications can improve a person's immune responses against Leishmania and reduce the risk of recurrence.
Prevention of Leishmaniasis
Leishmaniasis prevention begins with preventing sand fly bites.
For people who travel to or live in areas where the infection is common, the following can help:
Using insect repellents containing DEET (diethyltoluamide) on exposed skin
Wearing long-sleeved shirts, long pants, and socks
Avoiding outdoor activities from dusk to dawn, when sand flies are most active
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
Centers for Disease Control and Prevention: Leishmaniasis






