


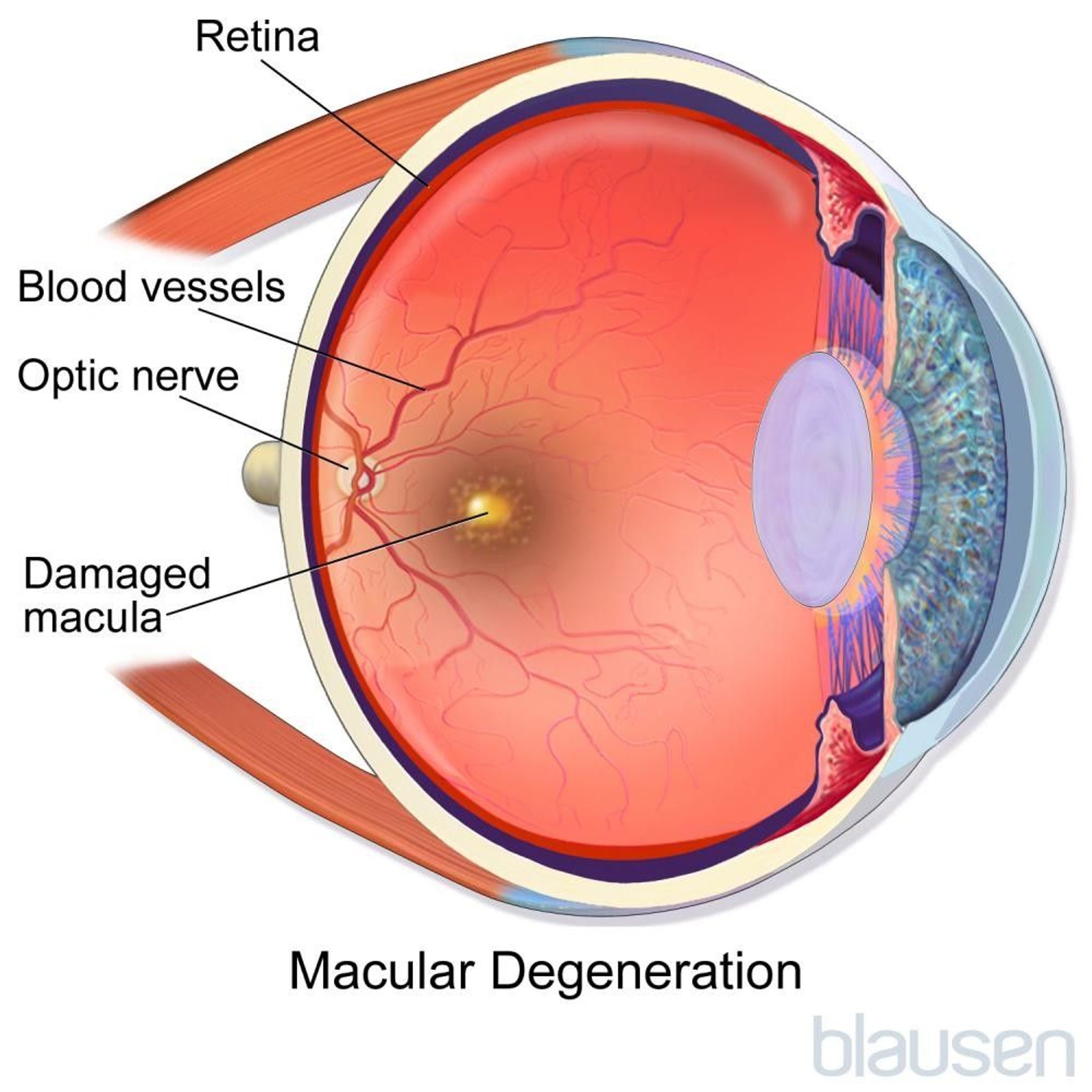
Age-related macular degeneration (AMD) causes progressive damage to the macula, the central and most vital area of the retina, resulting in gradual loss of central vision.
Central vision becomes washed out and loses detail, and straight lines may appear wavy.
Changes in the eye that characterize macular degeneration can often be identified by a doctor using specialized instruments during the examination.
Dietary supplements may help slow progression of the disorder.
Eye injections and laser treatments may be necessary for some people.
The retina is the transparent, light-sensitive structure at the back of the eye. The central area of the retina, called the macula, contains a high density of light-sensing cells. These cells produce the sharpest visual images and are responsible for central and color vision.


Age-related macular degeneration (AMD) is the most common cause of irreversible loss of central vision in older people. It is equally common among men and women. It is more common among White people.


Causes of AMD
The following are risk factors for age-related macular degeneration:
Age
Family history
Smoking
Certain genetic abnormalities
Cardiovascular disease (such as atherosclerosis)
Sun exposure
A diet low in omega-3 fatty acids (for example, in certain fish) and dark green leafy vegetables
Types
There are two types of AMD:
Dry (nonexudative or atrophic)
Wet (neovascular or exudative)
All AMD starts as the dry type. Some people (around 10%) go on to develop wet AMD. About 85% of people with AMD have only the dry type. Although relatively few people have the wet type, 80 to 90% of the severe vision loss caused by AMD results from the wet type.
Dry AMD causes the tissues of the macula to thin as cells disappear. Accumulated waste products from the rods and cones may produce deposits in the retina (the transparent, light-sensitive structure at the back of the eye) called drusen (yellow spots). Both eyes may be affected simultaneously in the dry form. There appears to be no scarring or bleeding or other fluid leakage in the macula.
Wet AMD develops when abnormal blood vessels grow in from the choroid (the layer of blood vessels that lies between the retina and the outer white layer of the eye called the sclera) under the macula and leak blood and fluid (hence the description as "wet"). Eventually, a mound of scar tissue develops under the macula. The wet form develops in one eye first but eventually may affect both eyes.
Symptoms of AMD
Dry AMD
In dry AMD, the loss of central vision occurs slowly and painlessly over years. People may have few or no symptoms but, when they do have symptoms, they often occur in both eyes. Objects may appear washed out, fine detail may be lost, and reading may become more difficult. As the disease progresses, central blind spots (scotomas) usually occur and can sometimes severely impair vision. Most people retain enough vision to read and drive.
Wet AMD
In wet AMD, loss of vision tends to progress quickly, usually over days or weeks, and may be even more sudden if one of the abnormal blood vessels bleeds. The first symptom may be an area of blurry, wavy, or distorted central vision. Vision at the outer edges of the visual field (peripheral vision) is typically not affected. Wet AMD usually affects one eye at a time. Often, difficulty with reading or watching television results.
AMD can severely damage vision and can lead to legal blindness in the affected eye.

Diagnosis of AMD
A doctor's examination of the eye
Doctors can usually diagnose age-related macular degeneration (AMD) by examining the eyes with ophthalmoscopy (shining a light through a magnifying lens and into the back of the eye). The retinal damage is almost always visible even before symptoms develop. To confirm the diagnosis of wet AMD, doctors may take color photographs of the retina or do . Optical coherence tomography, an imaging study, can often help make the diagnosis of wet AMD and assess how well the person is responding to treatment.
Treatment of AMD
Dietary supplements
Drugs and laser procedures
Low-vision aids and counseling
No treatment is currently available to undo damage caused by the dry type. No treatment is currently recommended for mild disease. Stopping smoking may help reduce the risk of developing age-related macular degeneration (AMD).
Dietary supplements
Dietary supplements are recommended for people with intermediate or advanced AMD in one eye. People can reduce their risk of developing advanced AMD by taking the following supplements:
Zinc
Vitamin C
Lutein plus zeaxanthin (for people who have smoked in the past or who currently smoke)
People who have used tobacco products within the past seven years should not take beta-carotene or vitamin A because these supplements can increase the risk of developing lung cancer. Lutein plus zeaxanthin can be used instead. Men who take these supplements have a higher risk of developing urinary tract and prostate problems, and women who take these supplements have a higher risk of developing stress incontinence. Beta-carotene may cause the skin to turn yellow.
Controlling risk factors for atherosclerosis (such as high blood pressure) and regularly eating more foods that have omega-3 fatty acids and eating more dark green leafy vegetables may help slow the progression of age-related macular degeneration. However, taking supplements of omega-3 fatty acids does not slow the progression of the disorder.
Drug treatments and laser procedures
the artery that supplies the retina) than other similar drugs.
Another treatment is photodynamic therapy. In this treatment, a substance that sensitizes the retinal blood vessels to laser light is injected into a vein in the arm, and then a beam of laser light is used to destroy the abnormal new blood vessels. If the new blood vessels are not directly under the macula, a thermal laser can be used to destroy them before they do more harm.
Surgery is rarely done for wet AMD.
Adjusting to vision loss
Magnifiers, high-power reading glasses, telescopic lenses, and closed-circuit television magnifying devices may help people with poor vision. Computer users can select from a variety of low-vision aids (see sidebar What Are Low-Vision Aids?). For example, one device projects an enhanced image from the computer onto an undamaged part of the retina. Certain types of software display computer data in large print or read the data aloud in a synthetic voice. Electronic books (e-books) may make reading easier because they allow people to adjust the font size and contrast level. For people with permanent, severe, central vision loss caused by AMD, an implantable miniature telescope can be used.
Counseling regarding the types of services that are available for people with poor vision is advisable and is typically given by a low-vision specialist (an ophthalmologist or optometrist who specializes in treating people with very poor vision).
More Information
The following are some English-language resources that may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Macular Degeneration Foundation: The latest information on age-related macular degeneration (AMD), including tips on healthy living and opportunities to support research on the prevention, treatment, and cure of AMD.
National Eye Institute: A resource for learning about eye health (in English and Spanish) for adults and children, as well as access to outreach campaigns. Simply type in the appropriate search term.
Prevent Blindness, Eye Diseases & Conditions: A wealth of information on AMD and other eye diseases that emphasizes treatment options (including nutritional supplements that may be useful in managing the condition), and tips on living with low vision.






