


Breast disorders may be noncancerous (benign) or cancerous (malignant). Most are noncancerous and not life threatening. Often, they do not require treatment. In contrast, breast cancer needs to be treated and may involve surgery or other intensive cancer treatments. Potential problems can often be detected early by the following:
Regular breast examinations with a health care professional
Mammograms as recommended
Early detection of breast cancer can be essential to successful treatment.
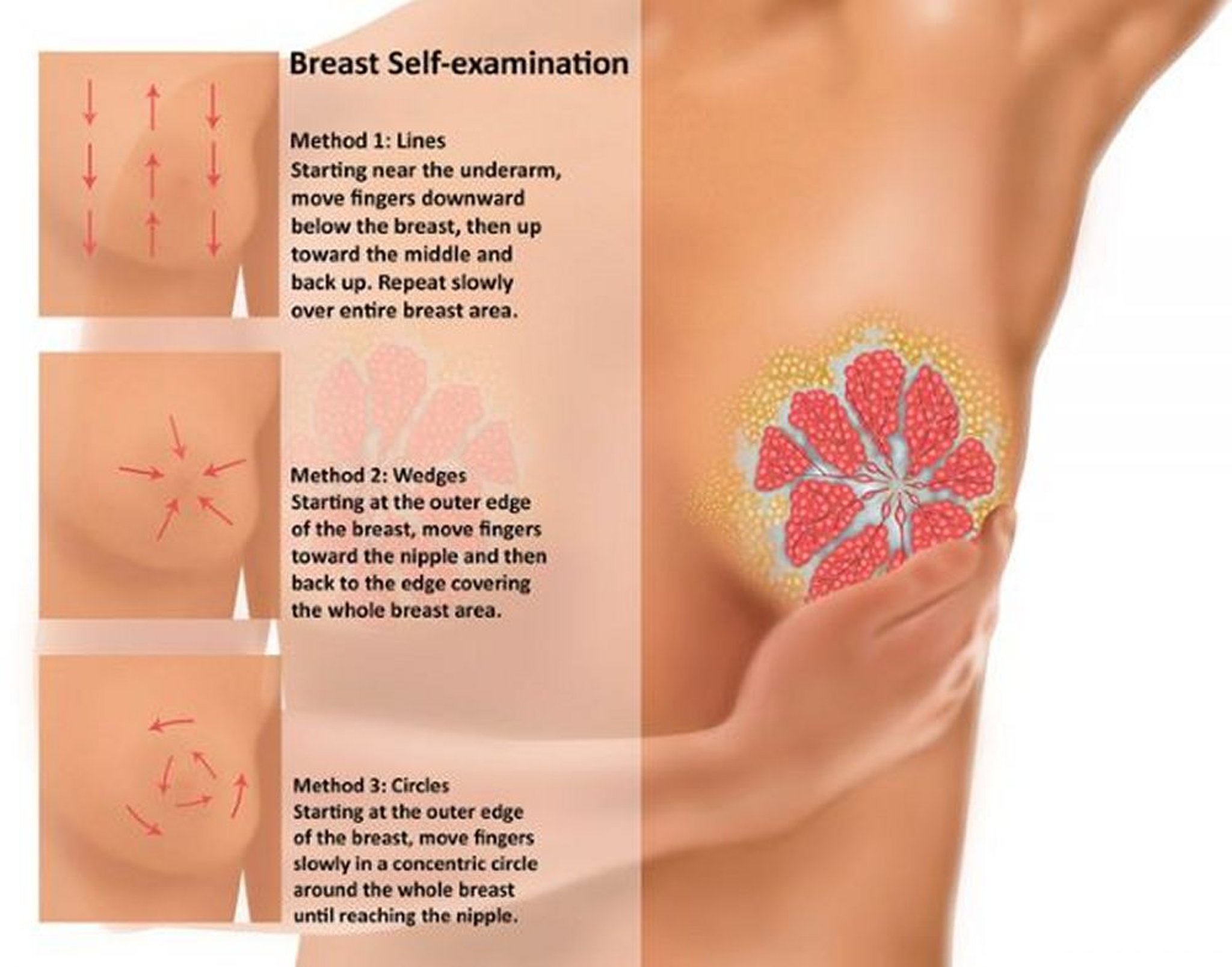
Women should be familiar with how their breasts and nipples normally look and feel. If a woman notices a change, she may want to do a breast self-examination. Women should report any changes to a health care professional right away. Most medical organizations no longer recommend monthly or weekly breast self-examinations as a routine way to check for cancer. Doing these examinations when there is no lump or other change does not help detect breast cancer early in women who get regular screening mammograms.
Rarely men develop breast cancer, and they should also be aware of changes in or around their nipples.
Symptoms of Breast Disorders
Symptoms related to the breast are common, leading to millions of visits to the doctor each year. These symptoms include
Changes in the breast skin (for example, the breast skin may become pitted, puckered, red, thickened, or dimpled)
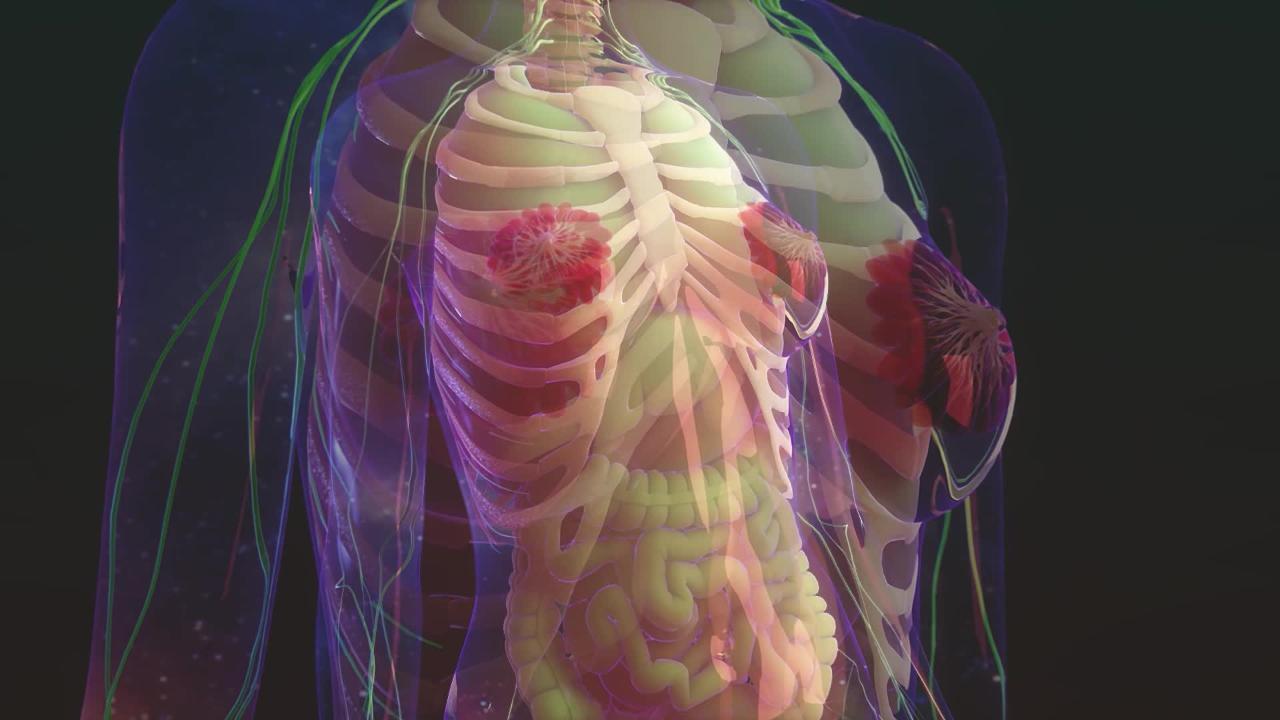
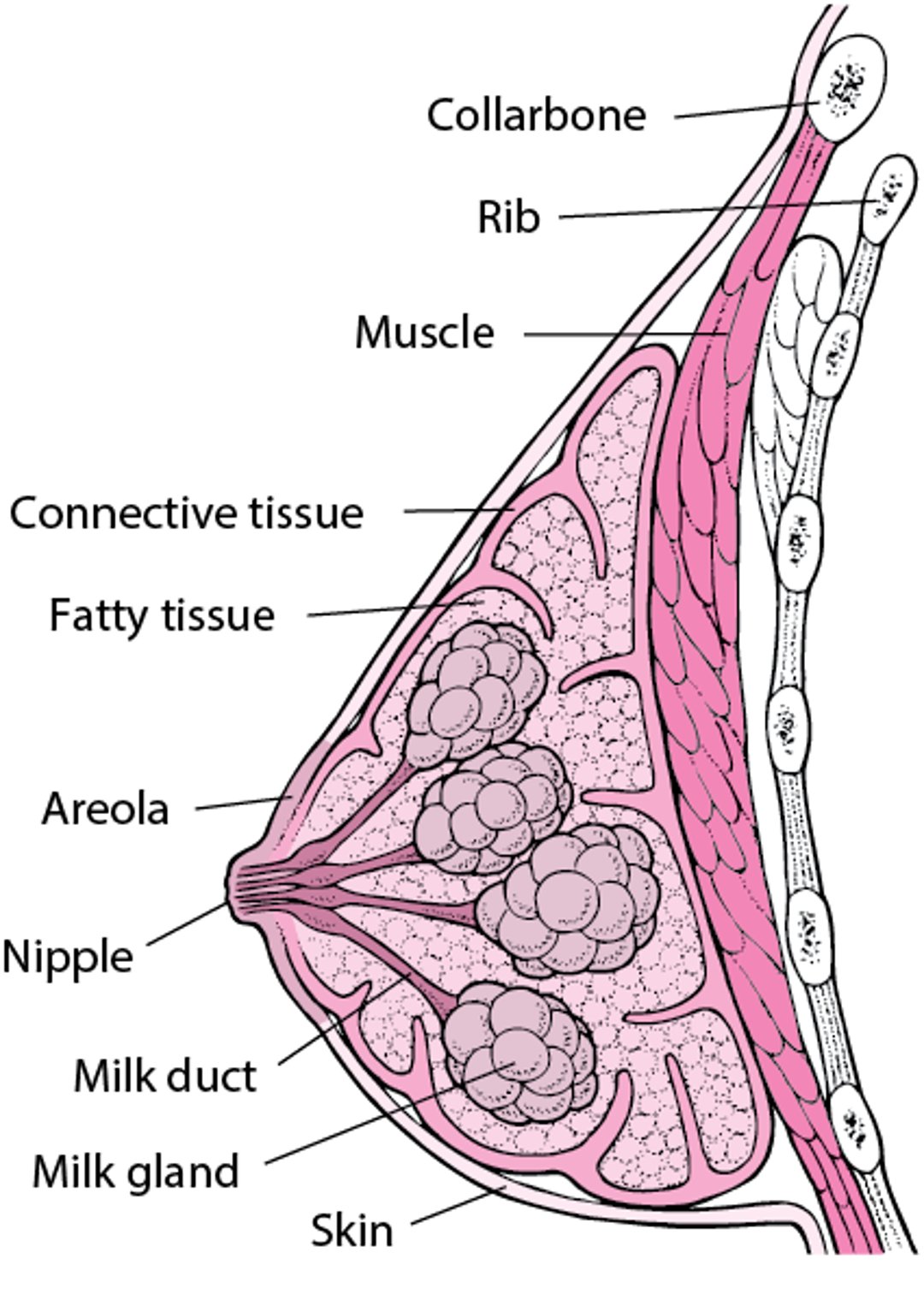
Inside the Breast
The female breast is composed of milk-producing glands (lobules) surrounded by fatty tissue and some connective tissue. Milk secreted by the glands flows through ducts to the nipple. Around the nipple is an area of pigmented skin called the areola. |

Breast symptoms do not necessarily mean that a woman has breast cancer or another serious disorder. For example, monthly breast tenderness that is related to hormonal changes before a menstrual period does not indicate a serious disorder.
However, women should see their doctor if they observe any change in a breast, particularly any of the following:
A lump or thickened area that feels distinctly different from other breast tissue
A lump that is stuck to the skin or chest wall
A lump that does not go away
Swelling that does not go away
Pitting, puckering, reddening, thickening, or dimpling in the skin of the breast
Scaly skin around the nipple
Changes in the shape of the breast
Changes in the nipple, such as being pulled inward
Discharge from the nipple, especially if it is bloody and/or occurs spontaneously (that is, without the nipple's being squeezed or stimulated by other means)
Evaluation of Breast Disorders
Doctors ask a woman about the symptoms she is having and other information related to possible causes, including
What the symptoms are
How long she has had the symptoms
Whether the symptoms occur at certain times of the month (related to the menstrual cycle)
Whether she has a discharge from the nipple, and if so, what it looks like and whether it was from one breast or both
Whether she is pregnant
What medications she is taking
Whether she or a family member has had breast cancer
When she had her last mammogram and what the results were
Breast examination
A breast examination is done. With a woman sitting or lying down, the doctor inspects each breast for irregularities in shape, a nipple that turns inward (inverted nipple), and lumps. The doctor also checks for dimpling, thickening, redness, or tightening of the skin over the breast. The doctor applies pressure around the nipples to check for a discharge. The discharge is examined to determine whether it contains blood. The armpits are checked for enlarged lymph nodes.
The doctor may examine the breast and armpits with a woman in different positions. For example, while sitting, she may be asked to press her palms together in front of the forehead. This position makes the chest muscles contract and makes subtle changes in the breast more noticeable.

Gwen Shockey/SCIENCE PHOTO LIBRARY
Testing
Imaging tests are used to
Check for breast abnormalities before they are noticed by a woman or her doctor (called breast cancer screening)
Evaluate abnormalities that have been identified, such as a breast lump found during the doctor's examination
Mammography involves taking x-rays of both breasts to check for abnormalities. A low dose of radiation is used. Only about 10 to 15% of abnormalities detected by mammography result from cancer.
Experts agree that all women should be screened for breast cancer. However, experts disagree about
When it should start
How often it should be done
When (or if) it should be stopped
Screening may include
Mammography
A breast examination by a health care professional
Magnetic resonance imaging (MRI) for high-risk patients
Screening mammography is usually started between the ages of 40 and 50 (see sidebar Breast Cancer: When to Start Screening?). Mammography is then done every 1 or 2 years. Experts have different recommendations about when to start routine mammography. Some experts recommend starting at age 50 because screening mammography is more accurate in women over age 50. Routine mammography may be stopped at age 75, depending on a woman's life expectancy and her wish for continued screening.
The types of tissue in the breast affect how well a mammogram can detect an abnormality. The breast contains fibroglandular tissue (composed of fibrous tissue and glands) and fatty tissue. As women age, the amount of fatty tissue in the breasts increases and the amount of fibroglandular tissue decreases. Abnormalities next to fatty tissue are easier to detect with a mammogram. That is why a mammogram becomes more accurate after age 50.
Some women have dense breasts. Having dense breasts means that women have more fibroglandular tissue and less fatty tissue. Abnormalities in dense breasts are harder to detect on a mammogram . Also, women with dense breasts have an increased risk of breast cancer. Thus, these women may require additional tests, such as breast ultrasonography, 3-dimensional mammography (tomosynthesis), or magnetic resonance imaging (MRI).
Mammography can be used to do the following:
Provide images of any abnormalities (such as a tumor or an abscess) and the tissues around the abnormality
Provide images of lymph nodes to check for abnormalities
Help doctors place a biopsy needle into abnormal tissue
After surgery, help doctors determine whether all the cancer was removed
Mammography may also be done if a woman or doctor finds a lump while examining the breasts or if a woman has breast pain or a discharge from the nipple.
Ultrasonography can be used to do the following:
Provide the first image of abnormalities that were detected during a breast examination in women under 30 years old
Provide more information about abnormalities detected by magnetic resonance imaging or mammography—for example, ultrasonography can show whether lumps are solid or filled with fluid (fluid-filled lumps—called cysts—are rarely cancerous)
Help doctors place a biopsy needle into abnormal tissue
Identify abnormal lymph nodes that may require biopsy
Magnetic resonance imaging (MRI) can be used to do the following:
Evaluate abnormal findings on breast examination or other imaging studies
After breast cancer is diagnosed, determine the size and number of the tumors, especially in women with dense breast tissue
Identify abnormal lymph nodes and thus help stage breast cancer
This information can help doctors plan surgery or other treatments for breast cancer.






