


Featured Content
Featured Content

Introduction to Eating Disorders
Eating disorders involve a persistent disturbance of eating or of behavior related to eating that Alters consumption or absorption of food Significantly impairs physical health and/or psychosocial...
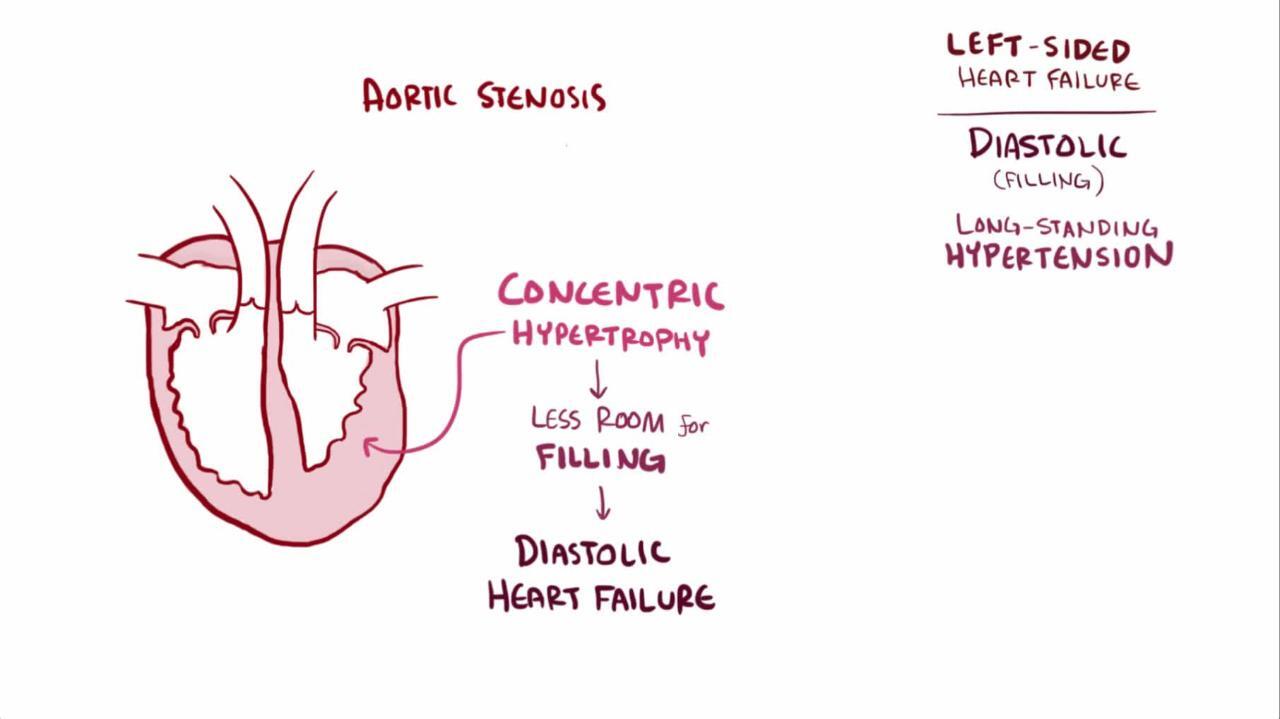
Heart Failure (HF)
Heart failure (HF) is a syndrome of ventricular dysfunction. Left ventricular (LV) failure causes shortness of breath and fatigue, and right ventricular (RV) failure causes peripheral and abdominal...

QUICK LINKS







Test Your Knowledge
View AllBreast Cancer
Which of the following is a correct statement about evaluating axillary lymph nodes in a patient with breast cancer?
- ALND is part of mastectomy procedures.
- Axillary lymph node dissection (ALND) is standard in all breast cancer surgery.
- Sentinel lymph node biopsy (SLNB), rather ALND, is usually done first.
- SLNB is done before ALND in mastectomy procedures.
LATEST NEWS
View All
PEARL OF THE DAY
PEARL OF THE DAY
Pneumothorax
Sudden hypotension in a mechanically ventilated patient should prompt consideration of tension pneumothorax. If the patient also has decreased breath sounds and hyperresonance to percussion, tension pneumothorax should be presumed and treated immediately without awaiting confirmation by chest x-ray.
Disclaimer
Important: The authors, reviewers, and editors of this material have made extensive efforts to ensure that treatments, drugs, and discussions about medical practice are accurate and conform to the standards accepted at the time of publication. However, constant changes in information resulting from continuing research and clinical experience, reasonable differences in opinions among authorities, unique aspects of individual clinical situations, and the possibility of human error in preparing such an extensive text mean that other sources of medical information may differ from the information on this site. The information on this site is not intended to be professional advice and is not intended to replace personal consultation with a qualified physician, pharmacist, or other health care professional. The reader should not disregard medical advice or delay seeking it because of something found on this site.
Content in the Manuals reflects medical practice and information in the United States. Outside of the United States, clinical guidelines, practice standards, and professional opinion may differ and the reader is advised to also consult local medical sources. Please note, not all content that is available in English is available in every language.





