


An atrial septal defect (ASD) is an opening in the interatrial septum, causing a left-to-right shunt and volume overload of the right atrium and right ventricle. Children are rarely symptomatic, but long-term complications after 20 years of age include pulmonary hypertension, heart failure, paradoxical emboli, and atrial arrhythmias. Adults and, rarely, adolescents may present with exercise intolerance, dyspnea, fatigue, and atrial arrhythmias. A soft midsystolic murmur at the upper left sternal border with wide and fixed splitting of the 2nd heart sound (S2) is common. Diagnosis is by echocardiography. Treatment is transcatheter device closure or surgical repair.
(See also Overview of Congenital Cardiovascular Anomalies.)
Atrial septal defects account for about 6 to 10% of cases of congenital heart disease (1). Most cases are isolated and sporadic, but some are part of a genetic syndrome (eg, mutations of chromosome 5, Holt-Oram syndrome). The combination of an atrial septal defect and atrioventricular conduction disturbance may be associated with a mutation in the NKX2-5 homeobox gene.
Classification
ASDs can be classified by location:
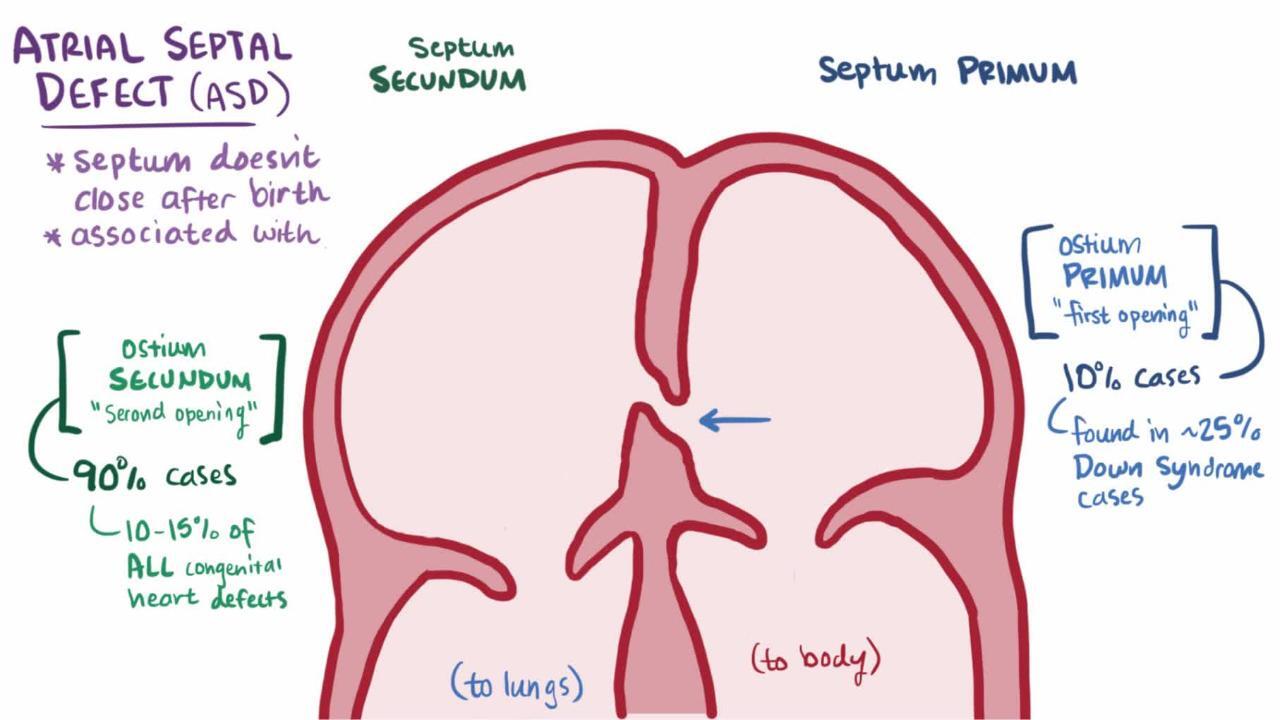
Ostium secundum: A defect in the fossa ovalis—in the center (or middle) part of the atrial septum
Sinus venosus: A defect in the posterior aspect of the septum, adjacent to the superior vena cava or inferior vena cava, and frequently associated with anomalous return of the right upper or lower pulmonary veins to the right atrium or vena cava
Ostium primum: A defect in the anteroinferior aspect of the septum, a form of atrioventricular septal defect (endocardial cushion defect)
General reference
1. Daubeney PEF, Rigby ML, Niwa K, Gatzoulis MA (eds): Pediatric Heart Disease: A Practical Guide. Wiley-Blackwell 2012 .
Pathophysiology of ASD
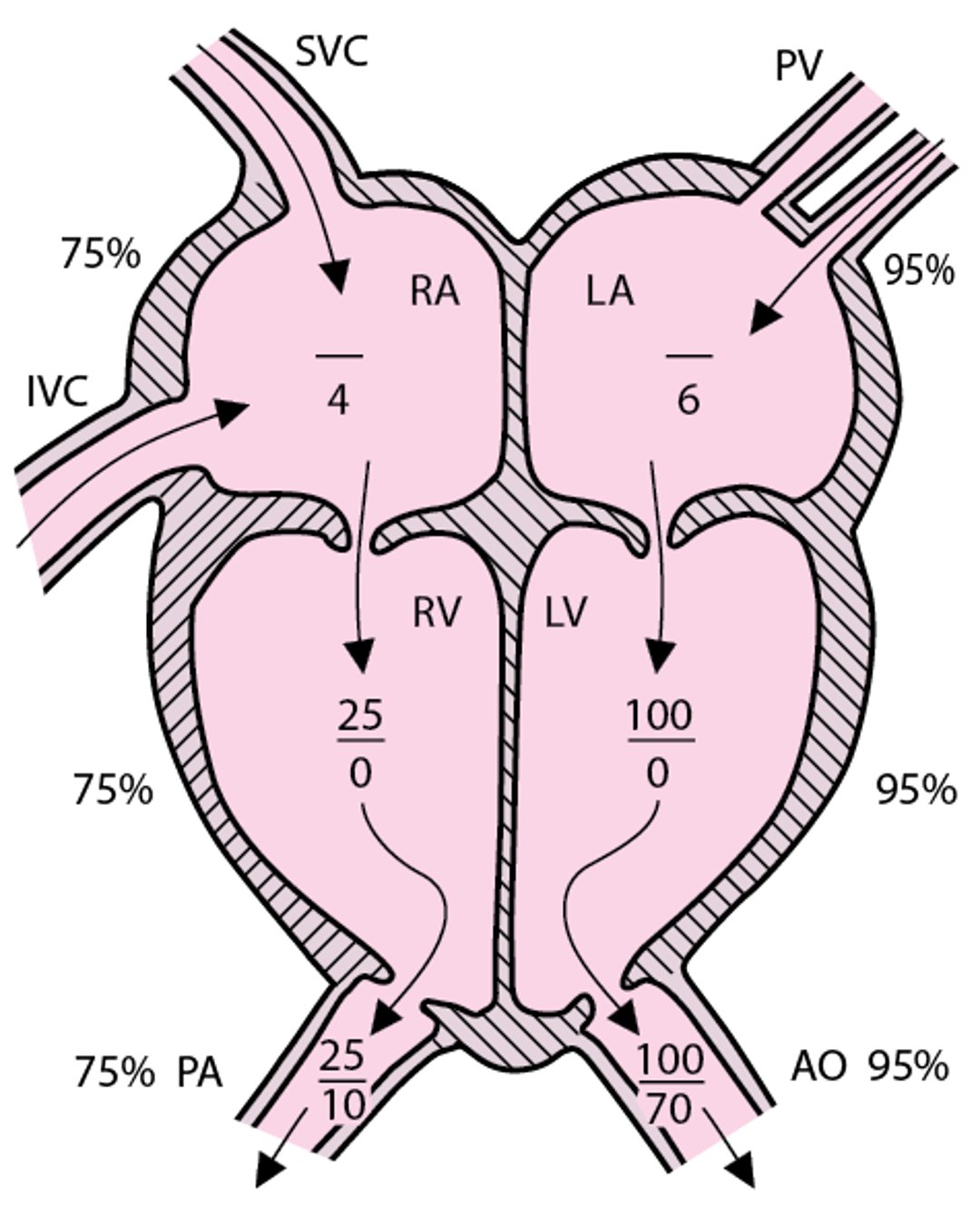
To understand hemodynamic changes and review normal hemodynamic data that occur in atrial septal defect (and other anomalies), see figure Normal circulation with representative right and left cardiac pressures.
Normal circulation with representative right and left cardiac pressures (in mm Hg)
Representative right heart oxygen saturation = 75%; representative left heart oxygen saturation = 95%. Atrial pressures are mean pressures. AO = aorta; IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PV = pulmonary veins; RA = right atrium; RV = right ventricle; SVC = superior vena cava. |

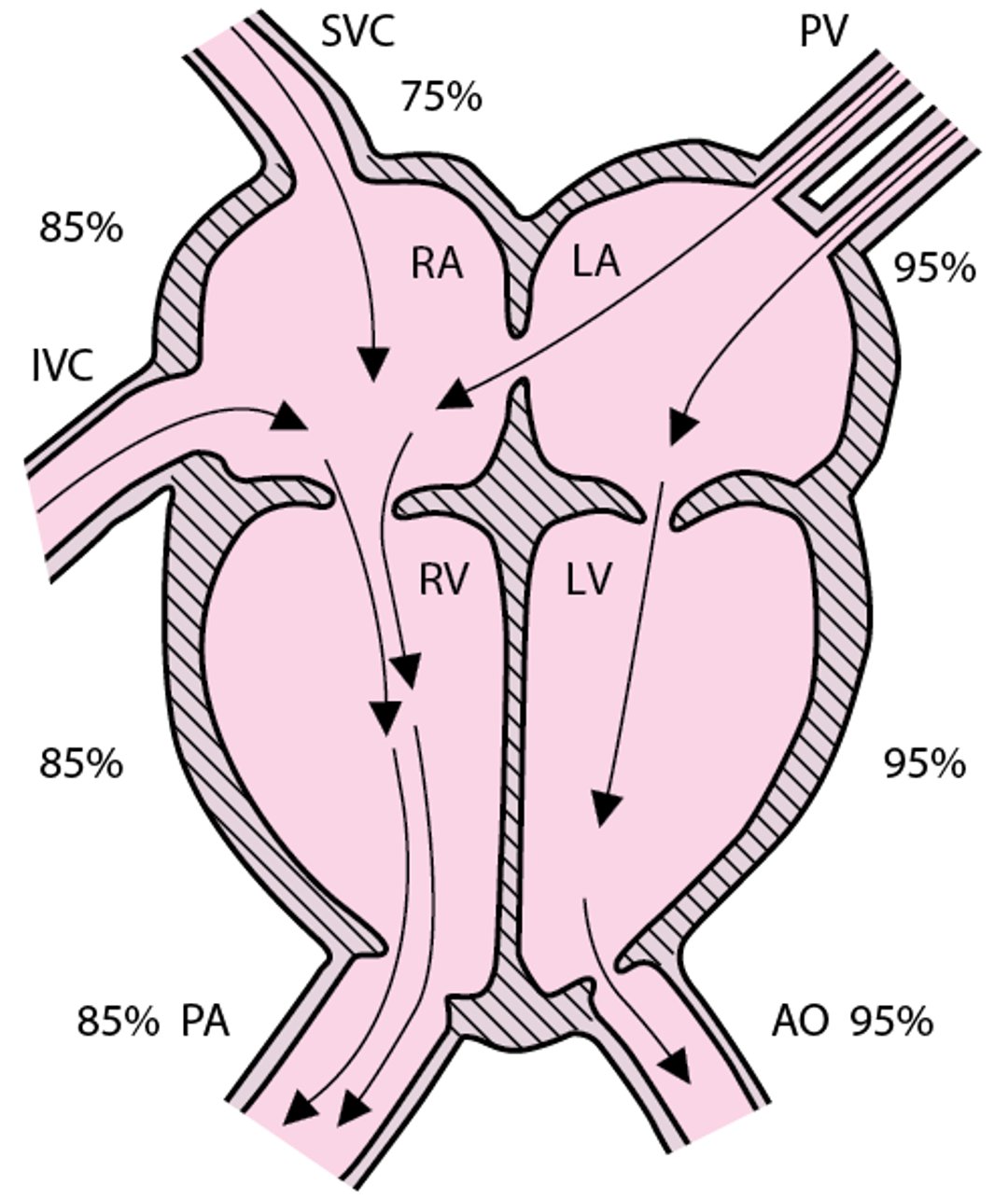
In atrial septal defect, shunting is left to right initially (see figure Atrial septal defect). Some small ASDs, often just a stretched patent foramen ovale, close spontaneously during the first few years of life. Persistent moderate to large ASDs result in large shunts, leading to right atrial and right ventricular volume overload. If unrepaired, these large shunts may lead to pulmonary artery hypertension, elevated pulmonary vascular resistance, and right ventricular hypertrophy by the time people are in their 30s or 40s. The absolute size of the defect in millimeters should not be taken in isolation, as the significance of the size of the defect varies with the age and size of the patient, and it is of lesser importance than the physiologic consequences of the degree of shunting through the defect (1). Atrial arrhythmias, such as supraventricular tachycardia (SVT), atrial flutter, or atrial fibrillation, may also occur. The presence of an atrial shunt, even if predominantly left-to-right, may be associated with a paradoxical embolus due to a transient right-to-left shunt. Ultimately, the increase in the pulmonary artery pressure and vascular resistance may result in a bidirectional atrial shunt with cyanosis (Eisenmenger syndrome) during mid to late adulthood (most commonly over the age of 40).
Atrial septal defect
Pulmonary blood flow and RA and RV volume are increased. (NOTE: Intracardiac pressures generally remain in the normal range throughout childhood.) With a large defect, RA and LA pressures are equal. AO = aorta; IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PV = pulmonary veins; RA = right atrium; RV = right ventricle; SVC = superior vena cava. |

Pathophysiology reference
1. McMahon CJ, Feltes TF, Fraley JK, et al: Natural history of growth of secundum atrial septal defects and implications for transcatheter closure. Heart 87(3):256-259, 2002. doi:10.1136/heart.87.3.256
Symptoms and Signs of ASD
Most patients with small or moderate-sized atrial septal defects are asymptomatic. Even large ASDs may not cause symptoms in young children. Larger shunts may cause slow weight gain in early childhood and exercise intolerance, dyspnea during exertion, fatigue, and/or palpitations in older patients. Passage of microemboli from the venous circulation across the ASD (paradoxical embolization), often associated with arrhythmias, may lead to cerebral or systemic thromboembolic events, such as stroke. Rarely, when an ASD is undiagnosed or untreated for decades, Eisenmenger syndrome develops.
Auscultation typically reveals a grade 2 to 3/6 midsystolic (ejection systolic) murmur (see table Heart Murmur Intensity) and a widely split, fixed S2 at the upper left sternal border in children. A large left-to-right atrial shunt may produce a low-pitched diastolic murmur (due to increased tricuspid flow) at the lower sternal borders. These findings may be absent in infants, even those who have a large defect. A prominent right ventricular cardiac impulse, manifested as a parasternal heave or lift, may be present.
Diagnosis of ASD
Chest x-ray and ECG
Echocardiography
Diagnosis of an atrial septal defect is suggested by cardiac examination, chest x-ray, and ECG and is confirmed by 2-dimensional echocardiography with color flow and Doppler studies.
If a significant shunt is present, ECG may show right axis deviation, right ventricular hypertrophy, or right ventricular conduction delay (an rSR′ pattern in V1with a tall R′). Chest x-ray shows cardiomegaly with dilation of the right atrium and right ventricle, a prominent main pulmonary artery segment, and increased pulmonary vascular markings.
Echocardiography confirms the presence of an ASD, defines the anatomic location and size of the defect, and assesses the degree of right atrial and right ventricular volume overload.
Cardiac catheterization is rarely necessary unless transcatheter closure of the defect is planned.
Treatment of ASD
Observation, transcatheter closure, or surgical repair
Most small (< 3 mm), centrally located atrial septal defects close spontaneously; many defects between 3 mm and 8 mm close spontaneously by age 3 years. These defects probably represent a stretched patent foramen ovale rather than true secundum ASDs. Ostium primum ASDs and sinus venosus ASDs do not close spontaneously.
Asymptomatic children with a small shunt require only observation and occasional echocardiography (typically about every 3 to 5 years). Although these children are theoretically at risk of paradoxical systemic embolization, this event is rare in childhood. Thus, it is not standard practice to close a small, hemodynamically insignificant defect.
Moderate-to-large ASDs (evidence of right ventricular volume overload on echocardiography) should be closed, typically between ages 2 years and 6 years. Repair may be considered earlier in children with chronic lung disease. Transcatheter closure with various commercial closure devices is possible in 85 to 90% of defects and is preferred when appropriate anatomic characteristics, such as adequate rims of septal tissue and distance from vital structures (eg, aortic root, pulmonary veins, tricuspid annulus), are present (1). Otherwise, surgical repair is indicated. Sinus venosus and ostium primum (atrioventricular septal type) defects are not amenable to device closure. If ASDs are repaired during childhood, perioperative mortality rate approaches 0, and long-term survival rates approach those of the general population.
Endocarditis prophylaxis is not needed preoperatively and is required only for the first 6 months after repair or if there is a residual defect adjacent to a surgical patch.
Treatment reference
1. Faccini A, Butera G: Atrial septal defect (ASD) device trans-catheter closure: limitations. J Thorac Dis 10 (Suppl 24):S2923–S2930, 2018.
Key Points
An atrial septal defect (ASD) is an opening in one of several parts of the interatrial septum, causing a left-to-right shunt.
Small atrial communications often close spontaneously, but larger ones do not, causing right atrial and ventricular overload and ultimately pulmonary artery hypertension, elevated pulmonary vascular resistance, and right ventricular hypertrophy; supraventricular tachycardia, atrial flutter, or atrial fibrillation may also occur.
ASDs can allow emboli from the veins to enter the systemic circulation (paradoxical embolization), causing arterial occlusion (eg, stroke).
Auscultation typically reveals a grade 2 to 3/6 midsystolic murmur and a widely split, fixed second heart sound; these findings may be absent in infants.
Moderate to large ASDs should be closed, typically between ages 2 years and 6 years, using a transcatheter device when possible.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers






