


Various rhythms result from supraventricular foci (usually in the atria). Diagnosis is by electrocardiography. Many are asymptomatic and require no treatment.
(See also Overview of Arrhythmias.)
Ectopic supraventricular rhythms include
Atrial premature beats
Atrial tachycardia
Multifocal atrial tachycardia
Nonparoxysmal junctional tachycardia
Wandering atrial pacemaker
Atrial premature beats
Atrial premature beats (APB), or premature atrial contractions (PAC), are common episodic impulses. They may occur in normal hearts with or without precipitating factors (eg, coffee, tea, alcohol, pseudoephedrine) or may be a sign of a cardiopulmonary disorder. They are common in patients with chronic obstructive pulmonary disease (COPD). They occasionally cause palpitations.
Diagnosis is by electrocardiography (ECG—see figure Atrial premature beat).
Atrial premature beat (APB)
In lead II, after the 2nd beat of sinus origin, the T wave is deformed by an APB. Because the APB occurs relatively early during the sinus cycle, the sinus node pacemaker is reset, and a pause—less than fully compensatory—precedes the next sinus beat. |



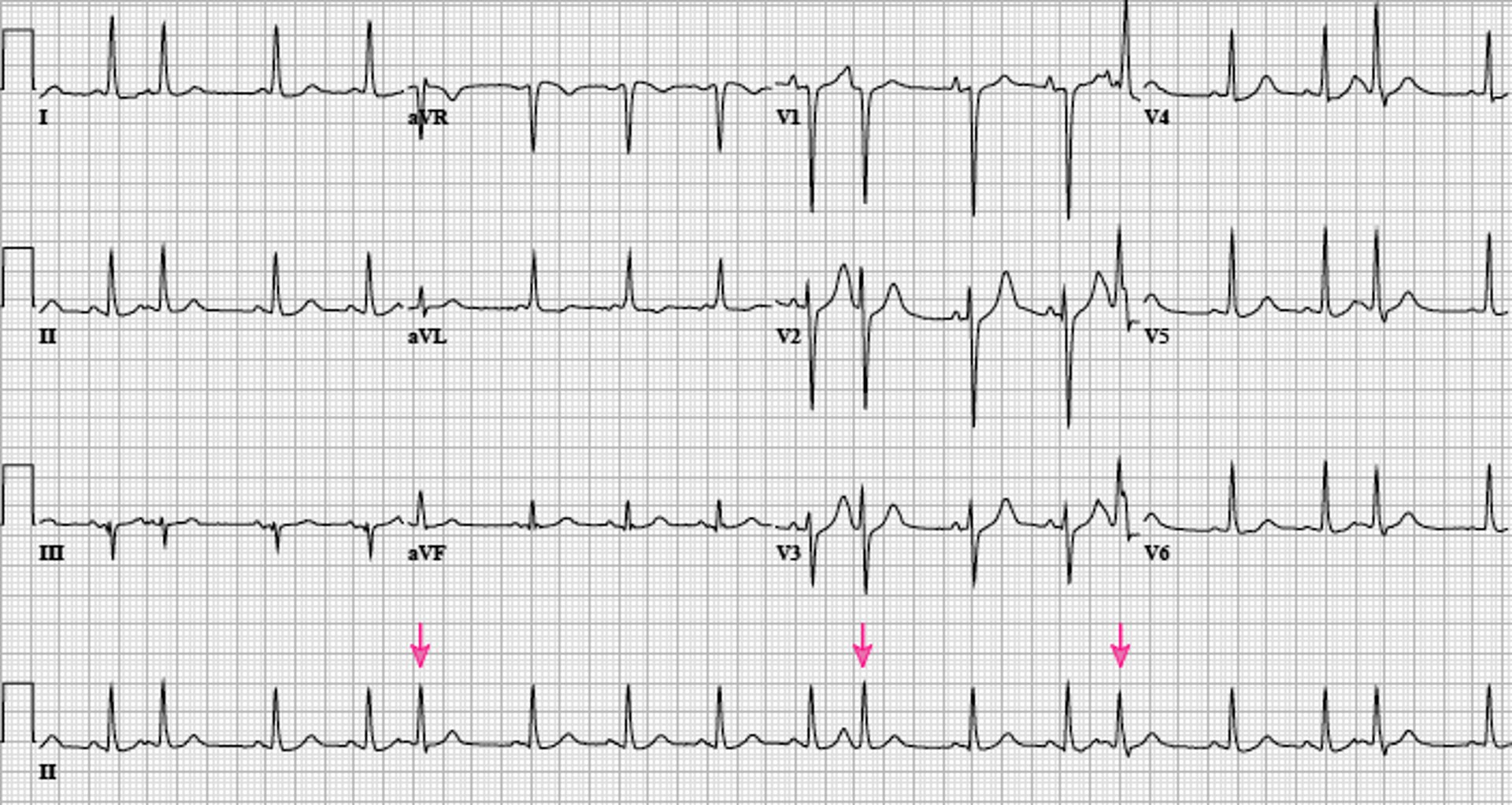
Image courtesy of L. Brent Mitchell, MD.
APBs may be normally, aberrantly, or not conducted and are usually followed by a noncompensatory pause. Aberrantly conducted APBs (usually with right bundle branch block morphology) must be distinguished from premature beats of ventricular origin.
Atrial escape beats are ectopic atrial beats that emerge after long sinus pauses or sinus arrest. They may be single or multiple; escape beats from a single focus may produce a continuous rhythm (called ectopic atrial rhythm). Heart rate is typically slower, P wave morphology is typically different, and PR interval is slightly shorter than in sinus rhythm.
Atrial tachycardia
Atrial tachycardia is a regular rhythm caused by the consistent, rapid atrial activation from a single atrial focus. Heart rate is usually 150 to 200 beats/minute; however, with a very rapid atrial rate, nodal dysfunction, and/or digitalis toxicity, atrioventricular (AV) block may be present, and ventricular rate may be slower. Mechanisms include enhanced atrial automaticity and intra-atrial reentry.
Atrial tachycardia is the least common form (5%) of paroxysmal supraventricular tachycardia and usually occurs in patients with a structural heart disorder. Other causes include atrial irritation (eg, pericarditis
Symptoms are those of other tachycardias (eg, light-headedness, dizziness, palpitations, and rarely syncope).
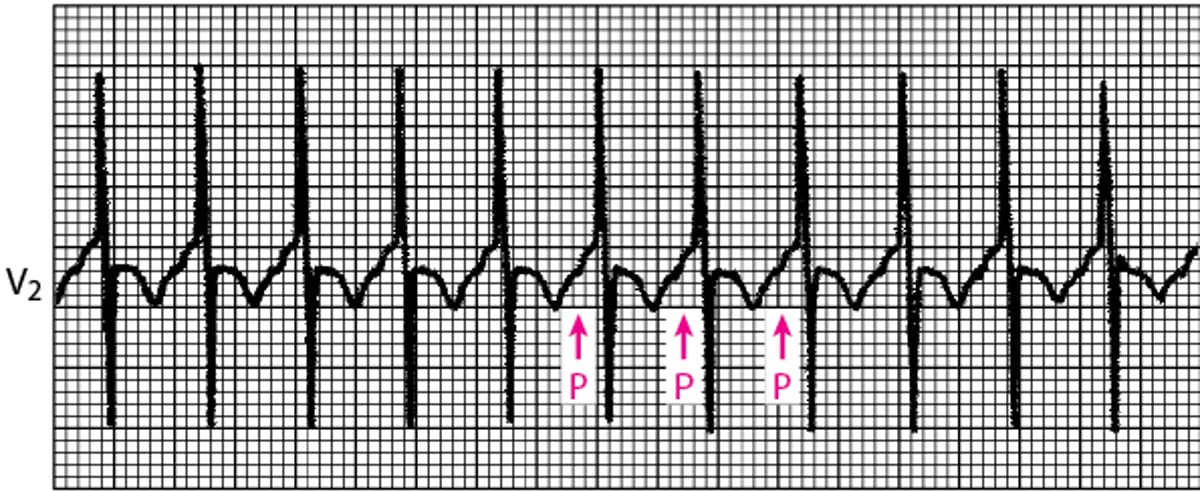
Diagnosis is by electrocardiography (ECG); P waves, which differ in morphology from normal sinus P waves, precede QRS complexes but may be hidden within the preceding T wave (see figure True atrial tachycardia).
True atrial tachycardia
This narrow QRS tachycardia arises from an abnormal automatic focus or intra-atrial reentry. P waves precede the QRS complexes; it is often a long RP interval tachycardia (PR < RP) but may be a short RP tachycardia (PR > RP) if atrioventricular nodal conduction is slow. |

Vagal maneuvers may be used to slow the heart rate, allowing visualization of P waves when they are hidden, but these maneuvers do not usually terminate the arrhythmia (demonstrating that the AV node is not an obligate part of the arrhythmia circuit).
Treatment involves managing causes and slowing ventricular response rate using a beta-blocker or calcium channel blocker. An episode may be terminated by direct current cardioversion. Pharmacologic approaches to termination and prevention of atrial tachycardia include antiarrhythmic drugs in class Ia, Ic, or III. If these noninvasive measures are ineffective, alternatives include overdrive pacing and ablation.
Multifocal atrial tachycardia
Multifocal atrial tachycardia (chaotic atrial tachycardia) is an irregularly irregular rhythm caused by the random discharge of multiple ectopic atrial foci. By definition, heart rate is > 100 beats/minute. On ECG, P-wave morphology differs from beat to beat, and there are ≥ 3 distinct P-wave morphologies. The presence of P waves distinguishes multifocal atrial tachycardia from atrial fibrillation. Except for the rate, features are the same as those of wandering atrial pacemaker. Symptoms, when they occur, are those of rapid tachycardia. Multifocal atrial tachycardia can be due to an underlying pulmonary disorder such as chronic obstructive pulmonary diseasecoronary artery disease, and electrolyte abnormalities such as hypokalemia. Treatment is directed at the underlying disorder.
Nonparoxysmal junctional tachycardia
Nonparoxysmal junctional tachycardia is caused by abnormal automaticity in the AV node or adjacent tissue, which typically follows open heart surgery, acute inferior myocardial infarction, myocarditis, or digitalis toxicity. Heart rate is 60 to 120 beats/minute; thus, symptoms are usually absent. ECG shows regular, normal-appearing QRS complexes without identifiable P waves or with retrograde P waves (inverted in the inferior leads) that occur shortly before (< 0.1 second) or after the QRS complex. The rhythm is distinguished from paroxysmal supraventricular tachycardia by the lower heart rate and gradual onset and offset. Treatment is directed at causes.
Wandering atrial pacemaker
Wandering atrial pacemaker (multifocal atrial rhythm) is an irregularly irregular rhythm caused by the random discharge of multiple ectopic atrial foci. By definition, heart rate is ≤ 100 beats/minute. Except for the rate, features are the same as those of multifocal atrial tachycardia. Treatment is directed at causes.






