


In Wolff-Parkinson-White syndrome, antegrade conduction occurs over an accessory pathway. If atrial fibrillation, develops this is a medical emergency as very rapid ventricular rates can develop.
(See also Overview of Arrhythmias and Atrial Fibrillation.)
In manifest Wolff-Parkinson-White (WPW) syndrome, antegrade conduction occurs over the accessory pathway. If atrial fibrillation develops, the normal rate-limiting effects of the atrioventricular (AV) node are bypassed, and the resultant excessive ventricular rates (sometimes 200 to 300 beats/minutes) may lead to ventricular fibrillation (see figure Atrial fibrillation in Wolff-Parkinson-White syndrome) and sudden death. Patients with concealed WPW syndrome are not at risk because in them, antegrade conduction does not occur over the accessory connection.
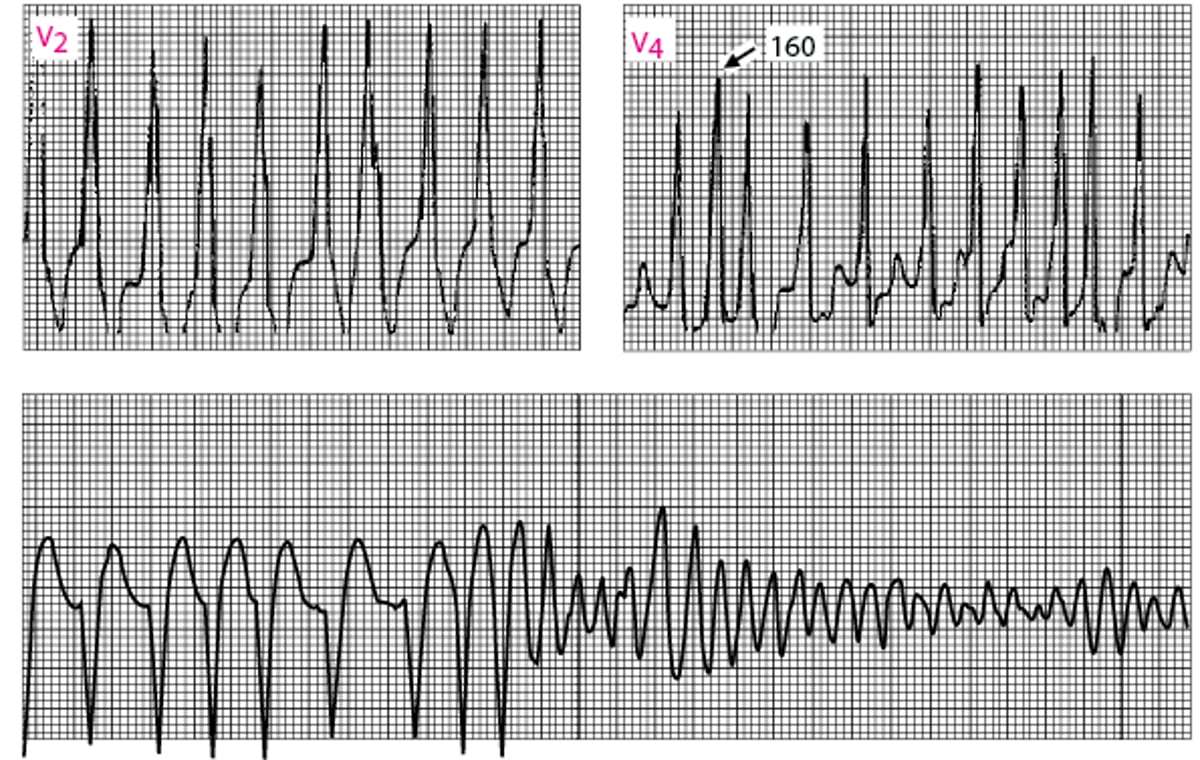
Atrial fibrillation in Wolff-Parkinson-White syndrome
Ventricular response is very fast (RR intervals minimum of 160 msec). Shortly thereafter, ventricular fibrillation develops (lead II continuous rhythm strip at bottom). |

Treatment of Atrial Fibrillation and WPW Syndrome
Direct-current cardioversion
The treatment of choice for Wolff-Parkinson-White syndrome with atrial fibrillation is direct current cardioversionantiarrhythmic drug can be used.
Pearls & Pitfalls






