


Coronary artery disease (CAD) involves impairment of blood flow through the coronary arteries, most commonly by atheromas. Clinical presentations include silent ischemia, angina pectoris, acute coronary syndromes (unstable angina, myocardial infarction), and sudden cardiac death. Diagnosis is by symptoms, ECG, stress testing, and sometimes coronary angiography. Prevention consists of modifying reversible risk factors (eg, hypercholesterolemia, hypertension, physical inactivity, obesity, diabetes, smoking). Treatment includes medications and procedures to reduce ischemia and restore or improve coronary blood flow.
Coronary artery disease is the leading cause of death in both sexes, accounting for approximately one third of all deaths, and substantial numbers of these occur in low resource areas (1). Mortality from coronary artery disease is approximately 5 times higher in men than in women, but the mortality difference declines with age (2).
General references
1. Ralapanawa U, Sivakanesan R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J Epidemiol Glob Health 2021;11(2):169-177. doi:10.2991/jegh.k.201217.001
2. Bots SH, Peters SAE, Woodward M. Sex differences in coronary heart disease and stroke mortality: a global assessment of the effect of ageing between 1980 and 2010. BMJ Glob Health 2017;2(2):e000298. Published 2017 Mar 27. doi:10.1136/bmjgh-2017-000298
Etiology of Coronary Artery Disease
Usually, coronary artery disease is due to
Coronary artery atherosclerosis: Subintimal deposition of atheromas in large and medium-sized coronary arteries
Less often, coronary artery disease is due to
Coronary artery spasm (see Vasospastic Angina)
Vascular endothelial dysfunction can promote atherosclerosis and contribute to coronary artery spasm. Endothelial dysfunction is also recognized as a cause of angina in the absence of epicardial coronary artery stenosis or spasm (see Microvascular Angina).
Rare causes include coronary artery embolism, dissection, aneurysm (eg, in Kawasaki disease), and vasculitis (eg, in Takayasu arteritis).
Pathophysiology of Coronary Artery Disease
Coronary atherosclerosis
Coronary atherosclerosis is often irregularly distributed in different vessels but typically occurs at points of turbulence (eg, vessel bifurcations). As the atheromatous plaque grows, the arterial lumen progressively narrows, resulting in ischemia (often causing angina pectoris). The degree of stenosis required to cause ischemia varies with oxygen demand.
Occasionally, an atheromatous plaque ruptures or splits. Reasons are unclear but probably relate to plaque morphology, plaque calcium content, and plaque softening due to an inflammatory process. Rupture exposes collagen and other thrombogenic material, which activate platelets and the coagulation cascade (see figure Pathways in Blood Coagulation), resulting in an acute thrombus, which interrupts coronary blood flow and causes some degree of myocardial ischemia. The consequences of acute ischemia, collectively referred to as acute coronary syndromes (ACS), depend on the location and degree of obstruction and range from unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI), to ST-segment elevation myocardial infarction (STEMI), which can result in transmural infarction, and other complications including malignant ventricular arrhythmias, conduction defects, heart failure, and sudden death.
Coronary artery spasm
Coronary artery spasm is a transient, focal increase in vascular tone, markedly narrowing the lumen and reducing blood flow; symptomatic ischemia (vasospastic angina) may result. Marked narrowing can trigger thrombus formation, causing infarction or life-threatening arrhythmia. Spasm can occur in arteries with or without atheroma.
In arteries without atheroma, basal coronary artery tone is probably increased, and response to vasoconstricting stimuli is probably exaggerated. The exact mechanism is unclear but may involve endothelial cell abnormalities of nitric oxide production or an imbalance between endothelium-derived contracting and relaxing factors.
In arteries with atheroma, the atheroma causes endothelial dysfunction, possibly resulting in local hypercontractility. Proposed mechanisms include loss of sensitivity to intrinsic vasodilators (eg, acetylcholine) and increased production of vasoconstrictors (eg, angiotensin II, endothelin, leukotrienes, serotonin, thromboxane) in the area of the atheroma. Recurrent spasm may damage the intima, leading to atheroma formation.
Use of vasoconstricting substances (eg, cocaine, nicotine) and emotional stress also can trigger coronary spasm.
Coronary artery dissection
Coronary artery dissection is a rare, non-traumatic tear in the coronary intima with creation of a false lumen. Blood flowing through the false lumen expands it, which restricts blood flow through the true lumen sometimes causing coronary ischemia or infarction. Dissection may occur in atherosclerotic or non-atherosclerotic coronary arteries. Non-atherosclerotic dissection is more likely in pregnant or postpartum females and/or patients with fibromuscular dysplasia or other connective tissue disorders.
Risk Factors for Coronary Artery Disease
Risk factors for coronary artery disease are the same as risk factors for atherosclerosis:
Older age
Male sex
Family history of early coronary artery disease (death from coronary artery disease in a first-degree relative prior to age 55 in males or age 65 in females)
High blood levels of low-density lipoprotein (LDL) cholesterol (see Dyslipidemia)
High blood levels of lipoprotein a
Low blood levels of high-density lipoprotein (HDL) cholesterol
Diabetes mellitus (particularly type 2)
Smoking (including secondhand exposure)
Obesity
Physical inactivity
High level of apoprotein B (apo B)
High blood levels of C-reactive protein (CRP)
Smoking may be a stronger predictor of myocardial infarction in females (1). Genetic factors play a role, and several systemic disorders (eg, hypertension, hypothyroidism) and metabolic disorders (eg, hyperhomocysteinemia) contribute to risk. A high level of apo B may identify increased risk when total cholesterol or LDL level is normal (2, 3).
High blood levels of C-reactive protein indicate plaque instability and inflammation and may be a stronger predictor of risk of ischemic events than high levels of LDL (4). High blood levels of triglycerides and insulin (reflecting insulin resistance) may be risk factors, but data are less clear. CAD risk is also increased by a diet high in fat and calories and low in phytochemicals (found in fruits and vegetables), fiber, and vitamins C, D, and E; by a diet relatively low in omega-3 (n-3) polyunsaturated fatty acids (PUFAs—at least in some people); and by poor stress management.
Risk factor references
1. Prescott E, Hippe M, Schnohr P, Hein HO, Vestbo J. Smoking and risk of myocardial infarction in women and men: longitudinal population study. BMJ 1998;316(7137):1043-1047. doi:10.1136/bmj.316.7137.1043
2. Sniderman AD, Thanassoulis G, Glavinovic T, et al. Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review. JAMA Cardiol 2019 Dec 1;4(12):1287-1295. doi: 10.1001/jamacardio.2019.3780
3. Wilkins JT, Li RC, Sniderman A, Chan C, Lloyd-Jones DM. Discordance Between Apolipoprotein B and LDL-Cholesterol in Young Adults Predicts Coronary Artery Calcification: The CARDIA Study. J Am Coll Cardiol 2016;67(2):193-201. doi:10.1016/j.jacc.2015.10.055
4. Ridker PM, Lei L, Louie MJ, et al. Inflammation and Cholesterol as Predictors of Cardiovascular Events Among 13 970 Contemporary High-Risk Patients With Statin Intolerance. Circulation 2024;149(1):28-35. doi:10.1161/CIRCULATIONAHA.123.066213
Coronary Artery Anatomy
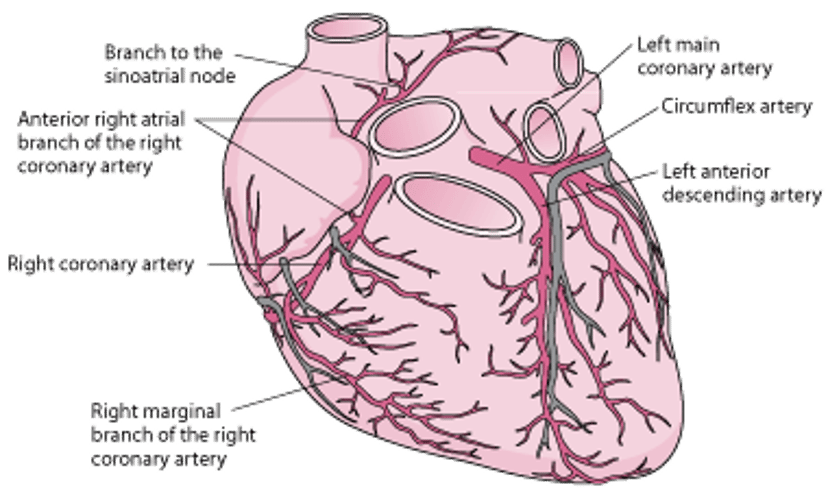
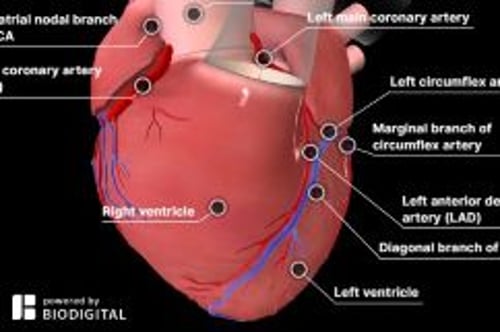
The right and left coronary arteries arise from the right and left coronary sinuses in the root of the aorta just above the aortic valve orifice (see figure Arteries of the Heart). The coronary arteries divide into large and medium-sized arteries that run along the heart’s surface (epicardial coronary arteries) and subsequently send smaller arterioles into the myocardium.
The left coronary artery begins as the left main artery and quickly divides into the left anterior descending (LAD), circumflex, and sometimes an intermediate artery (ramus intermedius). The LAD artery usually follows the anterior interventricular groove and, in some people, continues over the apex. This artery supplies the anterior septum (including the proximal conduction system) and the anterior free wall of the left ventricle (LV). The circumflex artery, which is usually smaller than the LAD artery, supplies the lateral LV free wall.
The dominant coronary artery refers to the one that gives rise to the posterior descending artery. Most people have right dominance: The right coronary artery passes along the atrioventricular (AV) groove over the right side of the heart; it supplies the sinus node (in 55%), right ventricle, and usually the AV node and inferior myocardial wall. About 10 to 15% of people have left dominance: The circumflex artery is larger and continues along the posterior AV groove to supply the posterior wall and AV node.
Arteries of the Heart

Treatment of Coronary Artery Disease
Medical therapy, including antiplatelet agents, lipid-lowering drugs (eg, statins), and beta-blockers
Percutaneous coronary intervention (PCI)
For acute thrombosis, sometimes fibrinolytic drugs
Coronary artery bypass grafting (CABG)
Treatment generally aims to reduce cardiac workload by decreasing oxygen demand and improving coronary artery blood flow, and, over the long term, to halt and reverse the atherosclerotic process. Coronary artery blood flow can be improved by percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). An acute coronary thrombosis may sometimes be dissolved by fibrinolytic drugs.
Medical therapy
(See also Medications for Acute Coronary Syndromes.)
Medical management of patients with CAD depends on symptoms, cardiac function, and the presence of other disorders. Recommended therapy includes
Antiplatelet agents to prevent thrombus formation
Statins to lower LDL cholesterol levels
Beta-blockers to reduce symptoms of angina
Antiplatelet agents and statins improve short-term and long-term outcomes, probably by improving atheromatous plaque stability and endothelial function.
Beta-blockers reduce symptoms of angina by reducing heart rate and contractility and decreasing myocardial oxygen demand. Beta-blockers also reduce mortality post-infarction, especially in the presence of post-myocardial infarction (MI) LV dysfunction.
Calcium channel blockers are also helpful. They often are combined with beta-blockers in managing angina and hypertension but have not been proven to reduce mortality.
Nitrates modestly dilate coronary arteries and decrease venous return, decreasing cardiac work and relieving angina quickly. Longer acting nitrate formulations help decrease angina events but do not decrease mortality.
Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) are most effective at reducing mortality post MI in CAD patients with LV dysfunction (1, 2).
Little evidence exists to guide therapy for patients with endothelial dysfunction. Treatment is generally similar to that for typical large-vessel atherosclerosis, and some evidence suggests that use of beta-blockers may enhance endothelial function (3).
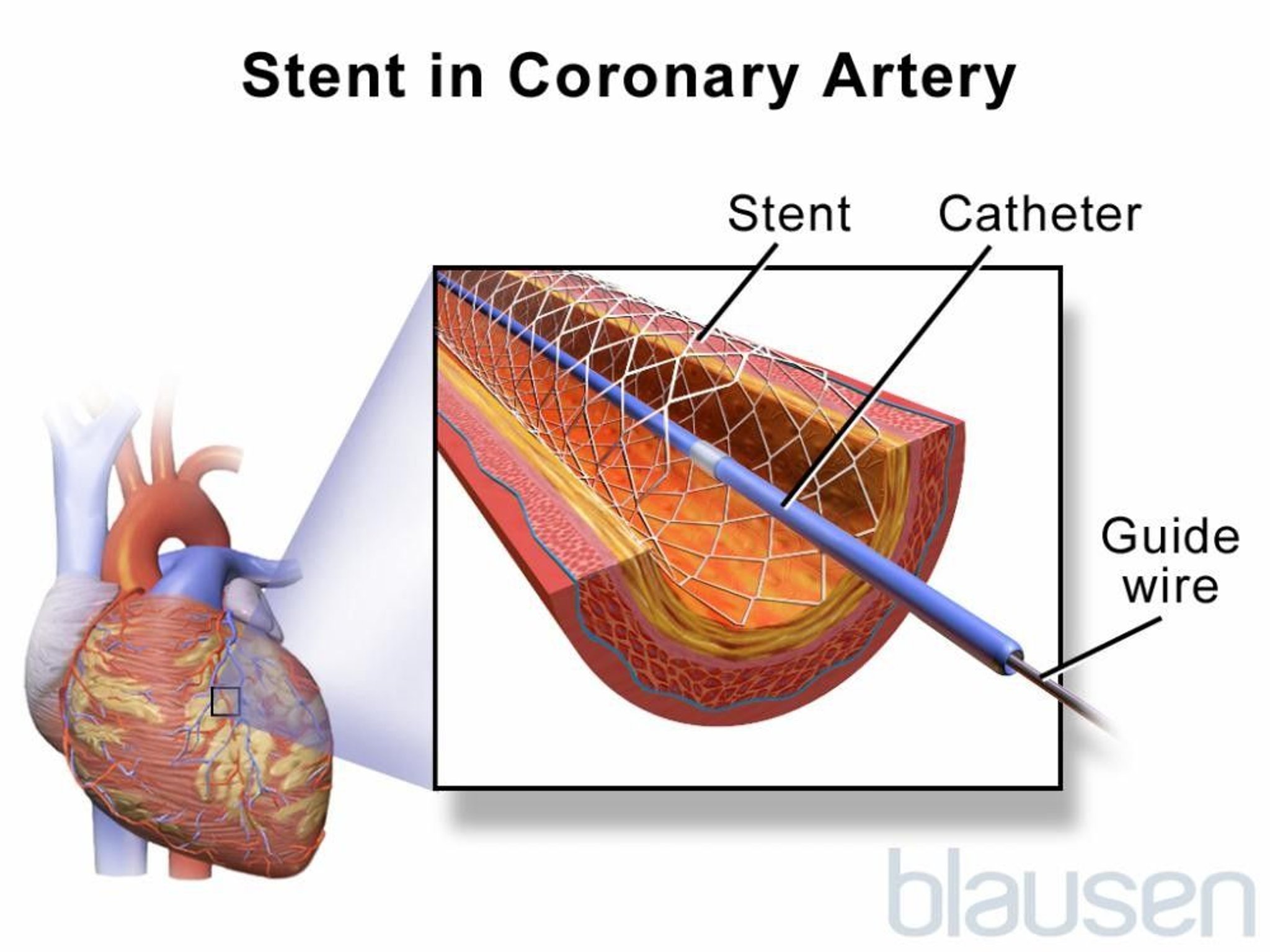
Percutaneous coronary intervention (PCI)
(See Percutaneous Coronary Interventions.)
PCI is indicated for patients with acute coronary syndrome (ACS) or with stable ischemic heart disease who have angina despite optimal medical therapy.
Drug-eluting stents,< 10% (4). Most PCI is done with stents, and most stents used in the United States are drug-eluting.
Patients without significant infarct or complications may return to work and usual activities usually within a few days after stent placement. However, cardiac rehabilitation is recommended for all patients.
In-stent thrombosis occurs because of the inherent thrombogenicity of metallic stents. Most cases occur within the first 24 to 48 hours. However, late stent thrombosis, occurring after 30 days and as late as ≥ 1 year (rarely), can occur with both bare-metal and drug-eluting stents, especially after cessation of antiplatelet therapy. Progressive endothelialization of the bare-metal stent occurs within the first few months and reduces the risk of thrombosis. However, the antiproliferative drugs released by drug-eluting stents inhibit this process and prolong the risk of thrombosis. Thus, patients who undergo stent placement are treated with various antiplatelet agents. The current standard regimen for patients with a bare-metal or drug-eluting stent consists of all of the following (5):

Glycoprotein IIb/IIIa inhibitors are not routinely used in stable patients (ie, no comorbidities, no acute coronary syndrome) having elective stent placement. They may be beneficial in some patients with an acute coronary syndrome but should not be considered routine. It is unclear whether it is beneficial to give glycoprotein IIb/IIIa inhibitors before arrival in the cardiac catheterization laboratory, but most national organizations do not recommend their use in this situation (5).
A statin is started after stent insertion, if one is not already being used because PCI by itself does not cure or prevent the progression of CAD. Statin therapy has been shown to improve long-term event-free survival (6). Patients who receive a statin before the procedure have a lower risk of periprocedural MI.
Overall, risks of undergoing PCI are comparable to those of CABG. Overall mortality rate is < 1%, but varies based on individual risk factors and tends to be similar to that of CABG; Q wave MI rate is < 1%. In < 1% of patients, intimal dissection causes obstruction requiring emergency CABG. Risk of stroke with PCI is lower than with CABG. A meta-analysis of 19 randomized trials reported a higher risk of stroke in patients undergoing CABG (1.2%) than PCI (0.34%,) at 30 days (7). Risk of bleeding is 1 to 2%.
Coronary artery bypass grafting (CABG)
(See Coronary Artery Bypass Grafting.)
CABG uses arteries (eg, internal mammary, radial) whenever possible, and if necessary, sections of autologous veins (eg, saphenous) to bypass diseased segments of the coronary arteries. At 1 year, about 85% of venous bypass grafts are patent, and after 5 years, one third or more are completely blocked. However, after 10 years, as many as 97% of internal mammary artery grafts are patent (8). Arteries also hypertrophy to accommodate increased flow. CABG is superior to PCI in patients with diabetes and in patients with multivessel disease amenable to grafting.
Coronary artery bypass grafting is typically done during cardiopulmonary bypass with the heart stopped; a bypass machine pumps and oxygenates blood. Risks of the procedure include stroke and MI. For patients with a normal-sized heart, no history of MI, good ventricular function, and no additional risk factors, risk is < 5% for perioperative MI, 1 to 2% for stroke, and ≤ 1% for mortality; risk increases with age, poor LV function, and presence of underlying disease. Operative mortality rate is 3 to 5 times higher for a second bypass than for the first.
After cardiopulmonary bypass, about 25 to 30% of patients develop cognitive dysfunction or behavioral changes, possibly caused by microemboli originating in the bypass machine (9). Cognitive or behavioral changes are more prevalent in older patients, prompting suspicion that these changes are most likely due to diminished "neuronal reserve," making older patients more susceptible to minor injuries incurred during cardiopulmonary bypass. Dysfunction ranges from mild to severe and may persist for weeks to years. To minimize this risk, some centers use a beating heart technique (off-pump CABG, which uses no cardiopulmonary bypass), in which a device mechanically stabilizes the part of the heart upon which the surgeon is working. However, long-term studies have failed to demonstrate lasting benefits of this approach in comparison to conventional on-pump CABG.
CAD may progress despite bypass surgery. Postoperatively, the rate of proximal obstruction of bypassed vessels increases. Vein grafts become obstructed early if thrombi form and later (several years) if atherosclerosis causes slow degeneration of the intima and media. Aspirin prolongs vein graft patency. Continued smoking has a profound adverse effect on patency. After CABG, a statin should be started or continued at maximally tolerated doses.
Treatment references
1. Indications for ACE inhibitors in the early treatment of acute myocardial infarction: systematic overview of individual data from 100,000 patients in randomized trials. ACE Inhibitor Myocardial Infarction Collaborative Group. Circulation 1998;97(22):2202-2212. doi:10.1161/01.cir.97.22.2202
2. Düsing R. Mega clinical trials which have shaped the RAS intervention clinical practice. Ther Adv Cardiovasc Dis 2016;10(3):133-150. doi:10.1177/1753944716644131
3. Peller M, Ozierański K, Balsam P, Grabowski M, Filipiak KJ, Opolski G. Influence of beta-blockers on endothelial function: A meta-analysis of randomized controlled trials. Cardiol J 2015;22(6):708-716. doi:10.5603/CJ.a2015.0042
4. Bønaa KH, Mannsverk J, Wiseth R, et al. Drug-Eluting or Bare-Metal Stents for Coronary Artery Disease. N Engl J Med 2016;375(13):1242-1252. doi:10.1056/NEJMoa1607991
5. Writing Committee Members, Lawton JS, Tamis-Holland JE, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol 2022 Apr 19;79(15):1547]. J Am Coll Cardiol 2022;79(2):e21-e129. doi:10.1016/j.jacc.2021.09.006
6. Grundy SM, Stone NJ, Bailey AL, et al: 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines [published correction appears in Circulation 2019 Jun 18;139(25):e1182-e1186] [published correction appears in Circulation 2023 Aug 15;148(7):e5]. Circulation 139(25):e1082–e1143, 2019. doi:10.1161/CIR.0000000000000625
7. Palmerini T, Biondi-Zoccai G, Reggiani LB, et al: Risk of stroke with coronary artery bypass graft surgery compared with percutaneous coronary intervention. J Am Coll Cardiol 60(9):798–805, 2012. doi:10.1016/j.jacc.2011.10.912
8. Hillis LD, Smith PK, Anderson JL, et al: 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines [published correction appears in Circulation 2011 Dec 20;124(25):e957]. Circulation 124(23):e652–e735, 2011. doi:10.1161/CIR.0b013e31823c074e
9. Kulik A, Ruel M, Jneid H, et al: Secondary prevention after coronary artery bypass graft surgery: a scientific statement from the American Heart Association. Circulation 131(10):927–964, 2015. doi:10.1161/CIR.0000000000000182
Prevention of Coronary Artery Disease
The American Heart Association (AHA) recommends using the pooled cohort risk assessment equations to estimate lifetime and 10-year risk of atherosclerotic cardiovascular disease. The risk calculator is based on sex, age, race, total and high-density lipoprotein (HDL) cholesterol levels, systolic blood pressure (and whether blood pressure is being treated), diabetes, and smoking status (1).
Prevention of coronary artery disease involves modifying atherosclerosis risk factors:
Weight loss
Healthful diet
Regular exercise
Modification of serum lipid levels
Reduction of salt intake
Control of hypertension
Control of diabetes
Antihypertensive recommendations vary. In the United States, for patients who are at low risk (< 10% 10-year risk) of atherosclerotic cardiovascular disease (ASCVD), antihypertensive therapy is recommended if blood pressure is > 130/80. In patients with coronary artery disease or whose risk of ASCVD is > 10%, antihypertensive medication is recommended for blood pressure > 130/80 mm Hg (2).
Modification of serum lipid levels (particularly with statins) may slow or even partially reverse the progression of CAD. Treatment goals have been modified. Instead of trying to achieve specific target low-density lipoprotein (LDL) cholesterol levels, patients are selected for treatment based on their risk of ASCVD. Lower risk patients with elevated LDL may not require statin treatment. Four higher risk patient groups have been identified in whom the benefit of statin therapy outweighs the risk of adverse events:
Patients with clinical ASCVD
Patients with LDL cholesterol ≥ 190 mg/dL (≥ 4.9 mmol/L)
Patients age 40 to 75 years with diabetes and LDL cholesterol levels of 70 to 189 mg/dL (1.8 to 4.9 mmol/L)
Patients age 40 to 75 years without diabetes, with LDL cholesterol levels of 70 to 189 mg/dL (1.8 to 4.9 mmol/L), and with ASCVD risk > 7.5%
Nicotinic acid or a fibrate may be added for patients with an HDL cholesterol level < 40 mg/dL (< 1.03 mmol/L), although several trials have failed to demonstrate a lower risk of ischemia or slowed progression of atherosclerosis when medications are used to raise HDL (3).
≥ 60 years (4). It can be considered for patients aged 40 to 59 years whose 10-year risk of cardiovascular disease exceeds 10%, but absolute benefit is likely to be small.
Prevention references
1. Arnett DK, Blumenthal RS, Albert MA, et al: 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 74:1376–1414, 2019. doi: 10.1016/j.jacc.2019.03.009
2. Whelton PB, Carey RM, Aronow WS, et al: ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 71:e127–e248, 2018. doi: 10.1161/HYP.0000000000000066
3. AIM-HIGH Investigators, Boden WE, Probstfield JL, Anderson T, et al: Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 365(24): 2255–2267, 2011. doi: 10.1056/NEJMoa1107579
4. US Preventive Services Task Force, Davidson KW, Barry MJ, et al: Aspirin Use to Prevent Cardiovascular Disease: US Preventive Services Task Force Recommendation Statement. JAMA 327(16):1577–1584, 2022. doi:10.1001/jama.2022.4983






