


Worldwide, about half a billion people (almost 8% of the world's population) have hearing loss (1). More than 10% of people in the US have some degree of hearing loss that compromises their daily communication, making it the most common sensory disorder. About 1/800 to 1/1000 neonates are born with severe to profound hearing loss. Two to 3 times as many are born with lesser hearing loss. During childhood, another 2 to 3/1000 children acquire moderate to severe hearing loss. Adolescents are at risk from excessive exposure to noise, head trauma, or both. Older adults typically experience a progressive decrease in hearing (presbycusis), which is directly related to a combination of aging, noise exposure, and genetic factors. It is estimated that about 30 million people in the US are exposed to injurious levels of noise on a daily basis.
Hearing deficits in early childhood can result in lifelong impairments in receptive and expressive language skills. The severity of the handicap is determined by
The age at which the hearing loss occurred
The nature of the loss (its duration, the frequencies affected, and the degree)
The susceptibilities of the individual child (eg, coexisting visual impairment, intellectual disability, primary language deficits, inadequate linguistic environment)
Children who have other sensory, linguistic, or cognitive deficiencies are affected most severely.
(See also Sudden Hearing Loss.)
General reference
1. Wilson BS, Tucci DL, Merson MH, et al: Global hearing health care: new findings and perspectives. Lancet 390(10111):2503-15, 2017. doi: 10.1016/S0140-6736(17)31073-5
Pathophysiology of Hearing Loss
Hearing loss can be classified as conductive, sensorineural, or both (mixed loss).
Conductive hearing loss occurs secondary to lesions in the external auditory canal, tympanic membrane (TM), or middle ear. These lesions prevent sound from being effectively conducted to the inner ear.
Sensorineural hearing loss is caused by lesions of either the inner ear (sensory) or the auditory (8th) nerve (neural). This distinction is important because sensory hearing loss is sometimes reversible and is seldom life threatening. A neural hearing loss is rarely recoverable and may be due to a potentially life-threatening brain tumor—commonly a cerebellopontine angle tumor. An additional type of sensorineural loss is termed auditory neuropathy spectrum disorder, when sound can be detected but the signal is not sent correctly to the brain, and is thought to be due to an abnormality of the inner hair cells or the neurons that innervate them within the cochlea (1).
Mixed loss may be caused by severe head injury with or without fracture of the skull or temporal bone, by chronic infection, or by one of many genetic disorders. It may also occur when a transient conductive hearing loss, commonly due to otitis media, is superimposed on a sensorineural hearing loss.
Differences Between Sensory and Neural Hearing Losses
Test | Sensory Hearing Loss | Neural Hearing Loss |
|---|---|---|
Speech discrimination | Moderate decrement | Severe decrement |
Discrimination with increasing sound intensity | Usually improves up to a point, depending on the severity and distribution of loss of sensory elements | Deteriorates |
Recruitment in which the perception of sound is exaggerated, especially at high sound levels | Present | Absent |
Acoustic reflex decay in which the acoustic reflex response is reduced over time during a measurement | Absent or mild | Present |
Waveforms in auditory brain stem responses | Well formed with normal latencies for mild to moderate hearing losses; reduced for more severe losses | Absent or with abnormally long latencies |
Otoacoustic emissions | Absent | Present |
Pathophysiology reference
1. Pham NS: The management of pediatric hearing loss caused by auditory neuropathy spectrum disorder. Curr Opin Otolaryngol Head Neck Surg 25(5):396-399, 2017. doi: 10.1097/MOO.0000000000000390
Etiology of Hearing Loss


Hearing loss can be
Congenital (see table Congenital Causes of Hearing Loss) or acquired (see table Some Causes of Acquired Hearing Loss)
Progressive or sudden
Temporary or permanent
Unilateral or bilateral
Mild or profound
The most common causes of hearing loss overall are the following:
Cerumen accumulation
Noise
Aging
Infections (particularly among children and young adults)
Cerumen (earwax) accumulation is the most common cause of treatable conductive hearing loss, especially in older patients. Foreign bodies obstructing the canal are sometimes a problem in children, both because of their presence and because of any damage inadvertently caused during their removal.
Noise can cause sudden or gradual sensorineural hearing loss. In acoustic trauma, hearing loss results from exposure to a single, extreme noise (eg, a nearby gunshot or explosion); some patients develop tinnitus as well. The loss is usually temporary (unless there is also blast damage, which may destroy the tympanic membrane, ossicles, or both). In noise-induced hearing loss, the loss develops over time because of chronic exposure to noise > 85 decibels (dB—see Sound Levels). Even before hearing loss can be documented, noise exposure can damage auditory neurons and their synapses on hair cells; this damage is referred to as "hidden hearing loss" or "synaptopathy," and patients may notice difficulty hearing in noisy environments and have accelerated age-related hearing loss (1). Although people vary somewhat in susceptibility to noise-induced hearing loss, nearly everyone loses some hearing if they are exposed to sufficiently intense noise for an adequate time. Repeated exposure to loud noise ultimately results in loss of hair cells in the organ of Corti. Hearing loss typically occurs first at 4 kHz and gradually spreads to the lower and higher frequencies as exposure continues. In contrast to most other causes of sensorineural hearing losses, noise-induced hearing loss may be less severe at 8 kHz than at 4 kHz.
Aging, together with noise exposure and genetic factors, is a common risk factor for progressive decrease in hearing. Age-related hearing loss is termed presbycusis. Presbycusis is due to a combination of sensory cell (hair cell) and neuronal loss. Research also strongly suggests that early noise exposure accelerates age-related hearing loss. Higher frequencies are more affected than lower frequencies in age-related hearing loss.
With more people wearing masks during the COVID-19 pandemic, many patients experienced an exacerbation of perceived hearing difficulty. This is the result of a reduced ability to read masked facial cues and lips, combined with the muffling of speech sounds from masked speakers.
Acute otitis media (AOM) is a common cause of transient mild to moderate hearing loss (mainly in children). However, without treatment, AOM sequelae and chronic otitis media (and the rarer purulent labyrinthitis) can cause permanent loss, particularly if a cholesteatoma forms.
Secretory otitis media (SOM) occurs in several ways. Almost all episodes of AOM are followed by a period of 2 to 4 weeks of SOM. SOM can also be caused by eustachian tube dysfunction (eg, resulting from cleft palate, benign or malignant tumors of the nasopharynx, or rapid changes in external air pressure as occur during descent from high altitudes or rapid ascent while scuba diving).
Autoimmune disorders can cause sensorineural hearing loss at all ages and can cause other symptoms and signs as well.
Ototoxic drugs can cause sensorineural hearing loss, and many also have vestibular toxicity.
Etiology reference
1. Liberman MC, Kujawa SG: Cochlear synaptopathy in acquired sensorineural hearing loss: manifestations and mechanisms. Hear Res 349:138-147, 2017. doi: 10.1016/j.heares.2017.01.003
Evaluation of Hearing Loss
Evaluation consists of detecting and quantifying hearing loss and determining etiology (particularly reversible causes).
Screening
Most adults and older children notice a sudden hearing loss, and caregivers may suspect that a neonate has a severe hearing loss within the first weeks of life when the neonate does not respond to voices or other sounds. However, progressive losses and nearly all losses in infants and young children must be detected by screening. Screening in children should begin at birth so that linguistic input can allow optimal language development. If screening is not done, severe bilateral losses may not be recognized until age 2 years, and mild to moderate bilateral or severe unilateral losses are often not recognized until children reach school age.
Screening in older people should be considered because patients may not have noticed a gradual decline in hearing or may think it a normal consequence of aging.
Suspected hearing loss at any time should prompt referral to a specialist.
History
History of present illness should note how long hearing loss has been perceived, how it began (eg, gradual, acute), whether it is unilateral or bilateral, and whether sound is distorted (eg, music is off—dull or lifeless) or there is difficulty with speech discrimination. The patient should be asked whether the loss followed any acute event (eg, head injury, loud noise exposure, barotrauma [particularly a diving injury], or starting of a drug). Important accompanying symptoms include other otologic symptoms (eg, ear pain, tinnitus, ear discharge), vestibular symptoms (eg, disorientation in the dark, vertigo), and other neurologic symptoms (eg, headache, weakness or asymmetry of the face, an abnormal sense of taste, fullness of the ear). In children, important associated symptoms include presence of delays in speech or language development, visual changes, or delayed motor development.
Review of systems should seek to determine the impact of hearing difficulty on the patient’s life.
Past medical history should note previous possibly causative disorders, including central nervous system infection, repeated ear infections, chronic exposure to loud noise, head trauma, rheumatic disorders (eg, rheumatoid arthritis, lupus), and a family history of hearing loss. Drug history should specifically query current or previous use of ototoxic drugs. For young children, a birth history should be sought to determine if there were any intrauterine infections or birth complications.
Physical examination
The focus is examination of the ears and hearing and the neurologic examination. The external ear is inspected for obstruction, infection, congenital malformations, and other lesions. The tympanic membrane (TM) is examined for perforation, drainage, otitis media (pus or fluid seen in the middle ear through the TM), and cholesteatoma. During the neurologic examination, particular attention needs to be paid to the 2nd through 7th cranial nerves as well as to vestibular and cerebellar function because abnormalities in these areas often occur with tumors of the brain stem and cerebellopontine angle. The Weber and Rinne tests require a tuning fork to differentiate conductive from sensorineural hearing loss.
In the Weber test, the stem of a vibrating 512-Hz or 1024-Hz tuning fork is placed on the midline of the head, and the patient indicates in which ear the tone is louder. In unilateral conductive hearing loss, the tone is louder in the ear with hearing loss. In unilateral sensorineural hearing loss, the tone is louder in the normal ear because the tuning fork stimulates both inner ears equally and the patient perceives the stimulus with the unaffected ear.
In the Rinne test, hearing by bone and by air conduction is compared. Bone conduction bypasses the external and middle ear and tests the integrity of the inner ear, 8th cranial nerve, and central auditory pathways. The stem of a vibrating tuning fork is held against the mastoid (for bone conduction); as soon as the sound is no longer perceived, the fork is removed from the mastoid, and the still-vibrating tines are held close to the pinna (for air conduction). Normally, the fork can once more be heard, indicating that air conduction is better than bone conduction. With conductive hearing loss over 25dB, the relationship is reversed; bone conduction is louder than air conduction. With sensorineural hearing loss, both air and bone conduction are reduced, but air conduction remains louder.
Red flags
Findings of particular concern are
Unilateral sensorineural hearing loss
Abnormalities of cranial nerves (other than hearing loss)
Rapidly worsening or sudden hearing loss
Interpretation of findings
Many causes of hearing loss (eg, cerumen, injury, significant noise exposure, infectious sequelae, drugs) are readily apparent based on results of the history and examination (see table Some Causes of Acquired Hearing Loss).
Associated findings are helpful in diagnosing the remaining small number of patients in whom no clear cause can be found. Patients who have focal neurologic abnormalities are of particular concern. The 5th or 7th cranial nerve or both are often affected by tumors that involve the 8th nerve, so loss of facial sensation and weak jaw clench (5th) and hemifacial weakness and taste abnormalities (7th) point to a lesion in that area. Signs of autoimmune disorders (eg, joint swelling or pain, eye inflammation) or renal dysfunction may suggest these disorders as a cause. Maxillofacial malformations may suggest a genetic or developmental abnormality.
All children with delays in speech or language development or difficulty in school should be evaluated for hearing loss. Intellectual disability, aphasia, and autism must also be considered. Delayed motor development may signal vestibular deficit, which is often associated with a sensorineural hearing loss.
Testing
Testing includes
Audiologic tests
Sometimes MRI or CT
Audiologic tests are required for all people who have hearing loss; these tests usually include
Measurement of pure-tone thresholds with air and bone conduction
Speech reception threshold
Speech discrimination
Tympanometry
Acoustic reflex testing
Information gained from these tests helps determine whether more definitive differentiation of sensory from neural hearing loss is needed.
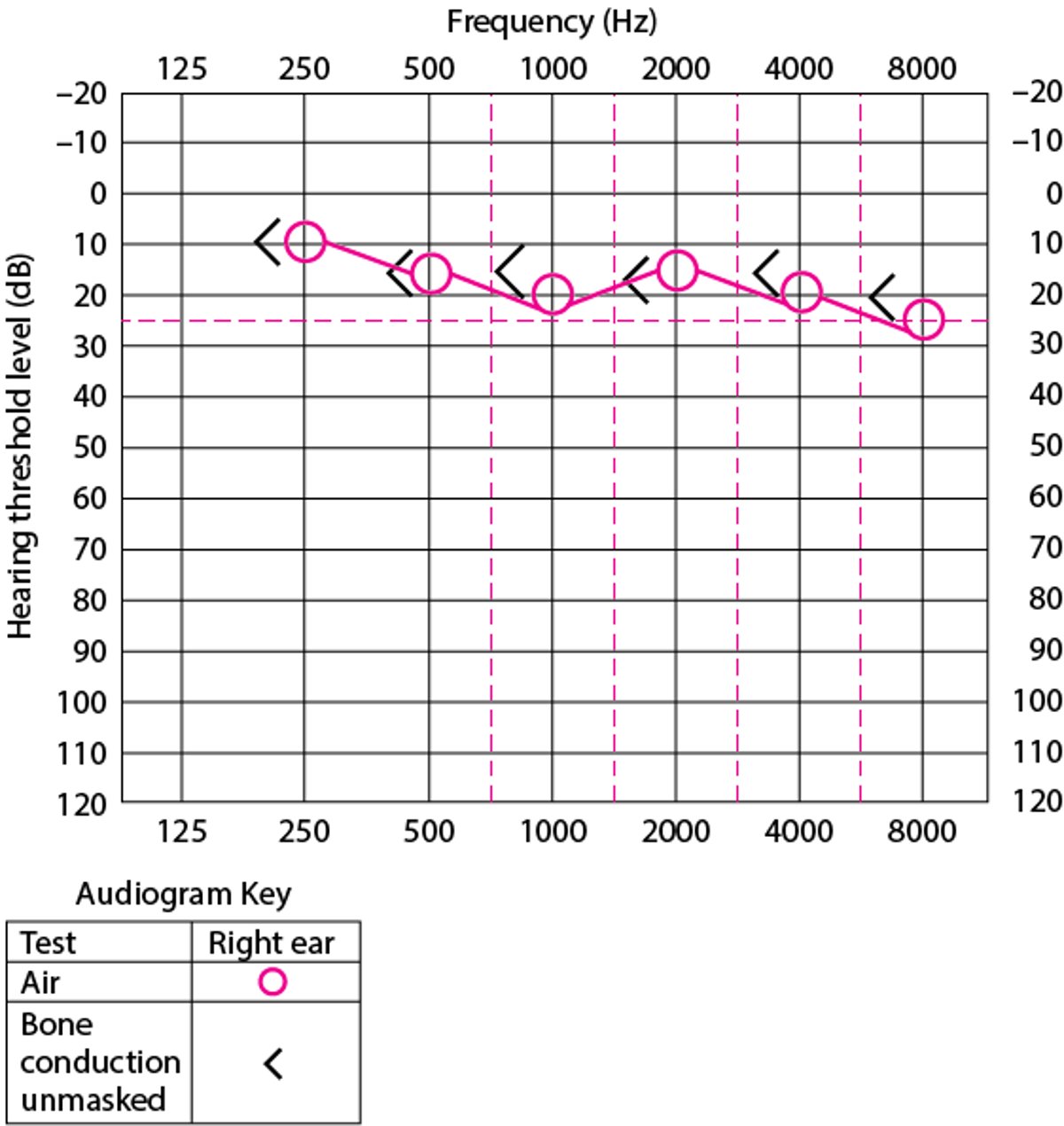
Pure-tone audiometry quantifies hearing loss. An audiometer delivers sounds of specific frequencies (pure tones) at different intensities to determine the patient’s hearing threshold (how loud a sound must be to be perceived) for each frequency. Hearing in each ear is tested from 125 or 250 to 8000 Hz by air conduction (using earphones) and up to 4 kHz by bone conduction (using an oscillator in contact with the mastoid process or forehead). Test results are plotted on graphs called audiograms (see figure Audiogram), which show the difference between the patient’s hearing threshold and normal hearing at each frequency. The difference is measured in dB. The normal threshold is considered 0 dB hearing level (Hl); hearing loss is considered present if the patient’s threshold is > 25 dB Hl. When hearing loss is such as to require loud test tones, intense tones presented to one ear may be heard in the other ear. In such cases, a masking sound, usually narrow band noise, is presented to the ear not being tested to isolate it.
Audiogram of right ear in a patient with normal hearing
Normal audiogram of the right ear. The vertical lines represent the frequencies that are tested from 125 to 8000 Hz. The horizontal lines record the threshold at which the patient states that the sound is heard. Normal thresholds are 0 dB +/− 10 dB. Patients with a hearing threshold below 20 dB are considered to have average or better-than-average hearing. The greater the dB, the louder is the sound and the worse the hearing. "O" is the standard symbol for air conduction of the right ear; "X" is the standard symbol for air conduction for the left ear. The "<" is the standard symbol for unmasked bone conduction for the right ear; ">" is the standard symbol for unmasked bone conduction of the left ear. The reason why both masked and unmasked measures are needed is to make sure one ear is not hearing the sound presented to the other ear (one ear is 'masked' so it does not hear the sound presented to the other ear, giving a false value). |

Speech audiometry includes the speech reception threshold (SRT) and the word recognition score. The SRT is a measure of the intensity at which speech is recognized. To determine the SRT, the examiner presents the patient with a list of words at specific sound intensities. These words usually have 2 equally accented syllables (spondees), such as "railroad," "staircase," and "baseball." The examiner notes the intensity at which the patient repeats 50% of the words correctly. The SRT approximates the average hearing level at speech frequencies (eg, 500 Hz, 1000 Hz, 2000 Hz).
The word recognition score tests the ability to discriminate among the various speech sounds or phonemes. It is determined by presenting 50 phonetically balanced one-syllable words at an intensity of 35 to 40 dB above the patient’s SRT. The word list contains phonemes in the same relative frequency found in conversational English. The score is the percentage of words correctly repeated by the patient and reflects the ability to understand speech under optimal listening conditions. A normal score ranges from 90 to 100%. The word recognition score is normal with conductive hearing loss, albeit at a higher intensity level, but can be reduced at all intensity levels with sensorineural hearing loss. Discrimination is even poorer in neural than in sensory hearing loss. Testing of words understood within full sentences is another type of recognition test that is often used to assess candidacy for implantable devices (when the benefit from hearing aids is insufficient).
Tympanometry measures the impedance of the middle ear to acoustic energy and does not require patient participation. It is commonly used to screen children for middle ear effusions. A probe containing a sound source, microphone, and air pressure regulator is placed snugly with an airtight seal into the ear canal. The probe microphone records the reflected sound from the tympanic membrane (TM) while pressure in the canal is varied. Normally, maximal compliance of the middle ear occurs when the pressure in the ear canal equals atmospheric pressure. Abnormal compliance patterns suggest specific anatomic disruptions. In eustachian tube obstruction and middle ear effusion, maximal compliance occurs with a negative pressure in the ear canal. When the ossicular chain is disrupted, as in necrosis or dislocation of the long process of the incus, the middle ear is excessively compliant. When the ossicular chain is fixed, as in stapedial ankylosis in otosclerosis, compliance may be normal or reduced.
The acoustic reflex is contraction of the stapedius muscle in response to loud sounds, which changes the compliance of the TM, protecting the middle ear from acoustic trauma. The reflex is tested by presenting a tone and measuring what intensity provokes a change in middle ear impedance as noted by movement of the TM. An absent reflex could indicate middle ear disease or a tumor of the auditory nerve. Any conductive hearing loss abolishes the acoustic reflex. Additionally, facial paralysis abolishes the reflex because the facial nerve innervates the stapedius muscle.
Advanced testing is sometimes needed. Gadolinium-enhanced MRI of the head to detect lesions of the cerebellopontine angle may be needed in patients with an abnormal neurologic examination or those whose audiologic testing shows poor word recognition, asymmetric sensorineural hearing loss, or a combination when the etiology is not clear.
CT is done if bony tumors or bony erosion is suspected. Magnetic resonance angiography and venography is done if vascular abnormalities such as glomus tumors are suspected.
The auditory brain stem response uses surface electrodes to monitor brain wave response to acoustic stimulation in people who cannot otherwise respond.
Electrocochleography measures the activity of the cochlea and the auditory nerve with an electrode placed on or through the eardrum. It can be used to assess and monitor patients with dizziness, can be used in patients who are awake, and is useful in intraoperative monitoring.
Otoacoustic emissions testing measures sounds produced by outer hair cells of the cochlea in response to a sound stimulus usually placed in the ear canal. These emissions are essentially low-intensity echoes that occur with cochlear outer hair cell activation. Emissions are used to screen neonates and infants for hearing loss and to monitor the hearing of patients who are using ototoxic drugs
Central auditory evaluation measures discrimination of degraded or distorted speech, discrimination in the presence of a competing message in the opposite ear, the ability to fuse incomplete or partial messages delivered to each ear into a meaningful message, and the capacity to localize sound in space when acoustic stimuli are delivered simultaneously to both ears. This testing should be done on certain patients, such as children with a reading or other learning problem and older people who seem to hear but do not comprehend.
In children with hearing loss, additional testing should include an ophthalmologic examination because many genetic causes of deafness also cause ocular abnormalities. Children with unexplained hearing loss should also have an ECG to look for long QT syndrome and possibly also genetic testing.
Treatment of Hearing Loss
The causes of a hearing loss should be determined and treated. Ototoxic drugs should be stopped or the dose should be lowered unless the severity of the disease being treated (usually cancer or a severe infection) requires that the risk of additional ototoxic hearing loss be accepted. Attention to peak and trough drug levels is mandatory to help minimize risk and should be obtained in all patients. In patients with renal dysfunction, adjustments to drug dosages with close attention to peak and trough levels are required to minimize the risk of ototoxicity (eg, see dosing considerations for aminoglycoside antibiotics). There are some genetic abnormalities involving the mitochondria that increase the sensitivity to aminoglycoside antibiotics, and these can be identified with genetic screening.
Fluid from middle ear effusion can be drained by myringotomy and prevented from reaccumulating with the insertion of a tympanostomy tube. Benign growths (eg, enlarged adenoids, nasal polyps) and malignant tumors (eg, nasopharyngeal cancers, sinus cancers) blocking the eustachian tube or ear canal can be removed. Hearing loss caused by autoimmune disorders may respond to corticosteroids.
Damage to the tympanic membrane or ossicles or otosclerosis may require reconstructive surgery (eg. tympanoplasty with ossicular chain reconstruction; ossiculoplasty). Brain tumors causing hearing loss may in some cases be removed or radiated and hearing preserved.
Many causes of hearing loss have no cure, and treatment involves compensating for the hearing loss with hearing aids and, for severe to profound loss, a cochlear implant. In addition, various coping mechanisms may help.
Hearing aids
Amplification of sound with a hearing aid helps many people. Although hearing aids do not restore hearing to normal, they can significantly improve communication. Advances in amplification circuits provide a more natural, tonal quality to amplified sound and offer features of "smart," responsive amplification that takes into account the listening environment (eg, in noise-challenging and multi-talker environments). Physicians should encourage hearing aid use and help patients overcome a sense of social stigma that continues to obstruct use of these devices, perhaps by making the analogy that a hearing aid is to hearing as eye glasses are to seeing. Other factors that limit more widespread hearing aid use include cost and comfort issues.
All hearing aids have a microphone, amplifier, speaker, earpiece, and volume control, although they differ in the location of these components. An audiologist should be involved in selection and fitting of a hearing aid.
The best models are adjusted to a person’s particular pattern of hearing loss. For example, people with mainly high-frequency hearing loss might not benefit from simple amplification, which merely makes the garbled speech they hear sound louder; they usually need a hearing aid that selectively amplifies the high frequencies. Some hearing aids contain vents in the ear mold, which facilitate the passage of high-frequency sound waves. Some use digital sound processing with multiple frequency channels so that amplification more precisely matches hearing loss as measured on the audiogram.
Telephone use can be difficult for people with hearing aids. Typical hearing aids cause squealing when the ear is placed next to the phone handle. Some hearing aids have a phone coil with a switch that turns the microphone off and links the phone coil electromagnetically to the speaker magnet in the phone.
For moderate to severe hearing loss, a postauricular (ear-level) aid, which fits behind the pinna and is coupled to the ear mold with flexible tubing, is appropriate. An in-the-ear aid is contained entirely within the ear mold and fits less conspicuously into the concha and ear canal; it is appropriate for mild to moderate hearing loss. Some people with mild hearing loss limited to high frequencies are most comfortably fitted with postauricular aids and completely open ear canals. Canal aids are contained entirely within the ear canal and are cosmetically acceptable to many people who would otherwise refuse to use a hearing aid, but they are difficult for some people (especially older people) to manipulate.
The CROS aid (contralateral routing of signals) is occasionally used for severe unilateral hearing loss; a hearing-aid microphone is placed in the nonfunctioning ear, and sound is routed to the functioning ear through a wire or radio transmitter. This device enables the wearer to hear sounds from the nonfunctioning side, allowing for some limited capacity to localize sound. If the better ear also has some hearing loss, the sound from both sides can be amplified with the binaural CROS (BiCROS) aid.
The body aid type is appropriate for profound hearing loss. It is worn in a shirt pocket or a body harness and connected by a wire to the earpiece (the receiver), which is coupled to the ear canal by a plastic insert (ear mold).
A bone conduction aid may be used when an ear mold or tube cannot be used, as in atresia of the ear canal or persistent otorrhea. An oscillator is held against the head, usually over the mastoid, with a spring band, and sound is conducted through the skull to the cochlea. Bone conduction hearing aids require more power, introduce more distortion, and are less comfortable to wear than air conduction hearing aids. Some bone conduction aids (bone-anchored hearing aids or BAHAs) are surgically implanted in the mastoid process, avoiding the discomfort and prominence of the spring band.
Cochlear implants
Patients with advanced levels of hearing loss, including those with some residual (natural) hearing but who even with a hearing aid cannot understand more than half of the words contained in connected speech, may benefit from a cochlear implant. The surgery may result in loss of some residual hearing. However, even if residual hearing is lost, cochlear implants can greatly improve hearing, even in people who are profoundly deaf.

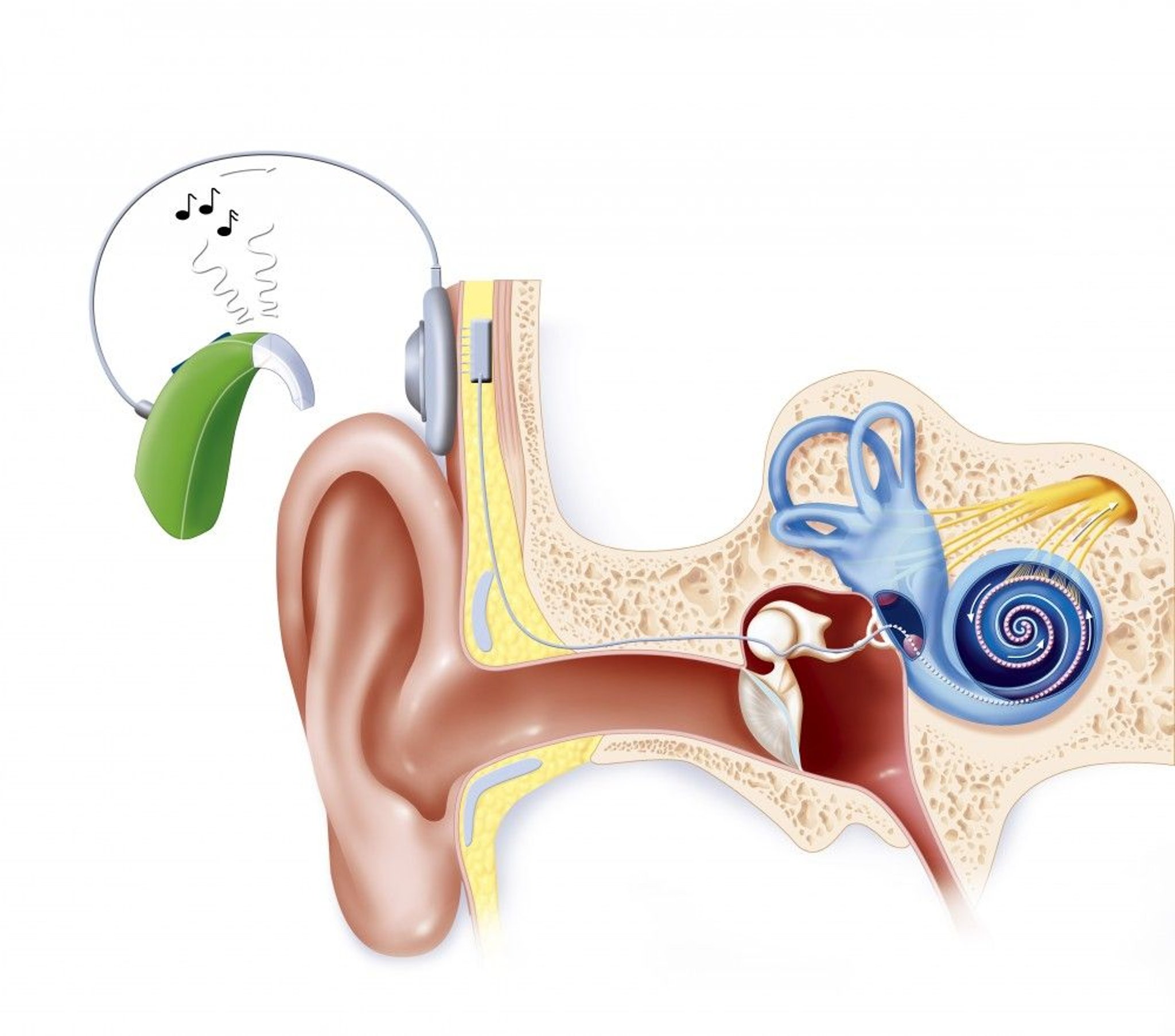
JACOPIN/BSIP/SCIENCE PHOTO LIBRARY
This device provides electrical signals directly into the auditory nerve via multiple electrodes implanted in the cochlea. An external microphone and processor convert sound waves to electrical impulses, which are transmitted through the skin electromagnetically from an external induction coil to an internal coil implanted in the skull above and behind the ear. The internal coil connects to electrodes inserted in the scala tympani.
Cochlear implants help with speech-reading by providing information about the intonation of words and the rhythm of speech. Many if not most adults with cochlear implants can discriminate words without visual clues, allowing them to talk on the telephone. Cochlear implants enable deaf people to hear and distinguish environmental sounds and warning signals. They also help deaf people modulate their voice and make their speech more intelligible.
Outcomes with cochlear implants vary, depending on a number of factors, including the
Length of time between onset of hearing loss and placement of the implant (shorter duration leads to better outcomes)
Cause of the underlying hearing loss
Position of the implant within the cochlea
Brain stem implants
Although cochlear implants are not an option for patients who have had both acoustic nerves destroyed (eg, by bilateral temporal bone fractures or neurofibromatosis) or are born without cochlear nerves, these patients can have some hearing restored by means of brain stem implants that have electrodes connected to sound-detecting and sound-processing devices similar to those used for cochlear implants, although usually not as good. In general, children born without cochlear nerves who receive the brain stem implant tend to have more hearing restored than patients who receive it following vestibular neuroma resection. Results of the brain stem implant range from assistance with lip-reading skills to the ability to understand language without lip-reading (termed 'open-set speech' understanding).
Assistive strategies and technologies
Alerting systems that use light let people know when the doorbell is ringing, a smoke detector is sounding, or a baby is crying. Special sound systems transmitting infrared or FM radio signals help people hear in theaters, churches, or other places where competing noise exists. Many television programs carry closed captioning. Telephone communication devices are also available.
Lip-reading or speech-reading is particularly important for people who can hear but have trouble discriminating sounds. Most people get useful speech information from lip-reading even without formal training. Even people with normal hearing can better understand speech in a noisy place if they can see the speaker. To use this information the listener must be able to see the speaker’s mouth. Health care personnel should be sensitive to this issue and always position themselves appropriately when speaking to the hearing-impaired. Observing the position of a speaker’s lips allows recognition of the consonant being spoken, thereby improving speech comprehension in patients with high-frequency hearing loss. Lip-reading may be learned in aural rehabilitation sessions in which a group of age-matched peers meets regularly for instruction and supervised practice in optimizing communication.
People can gain control over their listening environment by modifying or avoiding difficult situations. For example, people can visit a restaurant during off-peak hours, when it is quieter. They can ask for a booth, which blocks out some extraneous sounds. In direct conversations, people may ask the speaker to face them. At the beginning of a telephone conversation, they can identify themselves as being hearing-impaired. At a conference, the speaker can be asked to use an assistive listening system, which makes use of either inductive loop, infrared, or FM technology that sends sound through the microphone to a patient’s hearing aid.
People with profound hearing loss often communicate by using sign language. American Sign Language (ASL) is the most common version in the US. Other forms of linguistic communication that utilize visual inputs include Signed English, Signing Exact English, and Cued Speech. Around the world, it has been estimated that there are over 300 unique sign languages, with different countries, cultures, and villages having their own unique form of sign language.
Single-Sided Deafness
Patients with single-sided deafness (SSD) represent a special challenge. In one-on-one situations, hearing and speech understanding is relatively unaffected. However, with noisy backgrounds or complex acoustic environments (eg, classrooms, parties, meetings), patients with SSD are unable to hear and communicate effectively. Further, patients who hear out of only one ear are unable to localize the origin of sounds. The "head shadow" effect is the skull's ability to block sound coming from the deaf side from reaching the hearing ear. This can result in up to a 30 dB loss of sound energy reaching the hearing ear (as a comparison, a store-bought ear plug results in a 22 to 32 dB drop in hearing, roughly equivalent). For many patients, SSD can be life-altering and lead to significant disability at work and socially.
Treatment for SSD includes contralateral routing of signal (CROS) hearing aids or bone-anchored hearing implants that pick up sound from the deaf side and transfer it to the hearing ear without the loss of sound energy. Although these technologies improve hearing in noisy settings, they do not allow sound localization. Cochlear implants are increasingly being used with success in patients with SSD, particularly if the deaf ear also has severe tinnitus; implants have also been shown to provide sound localization.
Treatment of Hearing Loss in Children
In addition to treatment of any cause and the provision of hearing aids, children with hearing loss require support of language development with appropriate therapy. Because children must hear language to learn it spontaneously, most deaf children develop language only with special training, ideally beginning as soon as the hearing loss is identified (an exception would be a deaf child growing up with deaf parents who are fluent sign language users). Deaf infants must be provided with a form of language input. For example, a visually based sign language can provide a foundation for later development of oral language if a cochlear implant is not available. However, for children, there is no substitute for access to the sounds of speech (phonemes) to enable them to integrate acoustic inputs and develop a refined and nuanced understanding of speech and language.
If infants as young as 1 month have profound bilateral hearing loss and cannot benefit from hearing aids, they can be candidates for a cochlear implant. Although cochlear implants allow auditory communication in many children with either congenital or acquired deafness, they are generally more effective in children who already have developed language. Children who have postmeningitic deafness eventually develop an ossified inner ear that prevents the placement of an implant; they should receive cochlear implants as soon as possible to allow the implant to be correctly placed and maximize effectiveness. Children whose acoustic nerves have been destroyed by tumors may be helped by implantation of brain stem auditory-stimulating electrodes. Children with cochlear implants may have a slightly greater risk of meningitis than children without cochlear implants or adults with cochlear implants.
Children with unilateral deafness should be allowed to use a special system in the classroom, such as an FM auditory trainer. With these systems, the teacher speaks into a microphone that sends signals to a hearing aid in the child’s nonaffected ear, improving the child’s greatly impaired ability to hear speech against a noisy background.
Prevention of Hearing Loss
OSHA's occupational noise exposure standards). The louder the noise, the shorter the permissible time of exposure.
Geriatrics Essentials: Hearing Loss
Older people typically experience a progressive decrease in hearing (presbycusis). In the United States, 40% of those who are hearing impaired are older. Hearing impairment is prevalent in over one third of people over age 65 years and over half of people over age 75 years, making it the most common sensory disorder in this population. Nonetheless, hearing loss in older people should be evaluated and not ascribed simply to aging; older patients may have a tumor, a neurologic or autoimmune disorder, or an easily correctable conductive hearing loss. Also, recent research strongly suggests that hearing loss in older people can facilitate dementia, which may be mitigated by properly correcting hearing loss.
Presbycusis
Presbycusis is sensorineural hearing loss that probably results from a combination of age-related deterioration and cell death in various components of the hearing system and the effects of chronic noise exposure.
Hearing loss usually affects the highest frequencies (18 to 20 kHz) early on and gradually affects the lower frequencies; it usually becomes clinically significant when it affects the critical 2- to 4-kHz range at about age 55 to 65 (sometimes sooner). The loss of high-frequency hearing significantly affects speech comprehension. Although the loudness of speech seems normal, certain consonant sounds (eg, C, D, K, P, S, T) become harder to hear. Consonant sounds are the most important sounds for speech recognition. For example, when “shoe,” “blue,” “true,” “too,” or “new” is spoken, many people with presbycusis can hear the “oo” sound, but most have difficulty recognizing which word has been spoken because they cannot distinguish the consonants. This inability to distinguish consonants causes affected people to often think the speaker is mumbling. A speaker attempting to speak louder usually accentuates vowel sounds (which are low frequency), doing little to improve speech recognition. Speech comprehension is particularly difficult when background noise is present.
Screening
A screening tool is often helpful for older people because many do not complain of hearing loss. One tool is the Hearing Handicap Inventory for the Elderly–Screening Version, which asks
Does a hearing problem cause you to feel embarrassed when you meet people?
Does a hearing problem cause you to feel frustrated when talking to a family member?
Do you have difficulty hearing when someone whispers?
Do you feel handicapped by a hearing problem?
Does a hearing problem cause you difficulty when visiting friends, relatives, or neighbors?
Does a hearing problem cause you to attend religious services less often than you would like?
Does a hearing problem cause you to have arguments with family members?
Does a hearing problem cause you difficulty when listening to the television or radio?
Do you feel that any difficulty with your hearing hampers your personal or social life?
Does a hearing problem cause you difficulty when in a restaurant with relatives or friends?
Scoring is “no” = 0 points, “sometimes” = 2 points, and “yes” = 4 points. Scores > 10 suggest significant hearing impairment and necessitate follow-up.
Key Points
Cerumen, genetic disorders, infections, aging, and noise exposure are the most common causes of hearing loss.
All patients with hearing loss should have audiologic testing.
Cranial nerve deficits and other neurologic deficits should raise concern and warrant imaging tests.
Treatment modalities include correction of reversible causes, hearing aids, surgical procedures including ossicular reconstruction and cochlear implants, and various assistive technologies.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
National Institute on Deafness and Other Communication Disorders: Information for patients and providers regarding hearing loss and other communication disorders, spanning functions of hearing, balance, taste, smell, voice, speech, and language
Center for Disease Control and Prevention—Hearing Loss in Children: Information for parents about programs and services for children with hearing loss
The National Institute for Occupational Safety and Health (NIOSH)—Noise and Hearing Loss Prevention: Reviews occupational regulations and standards, noise control strategies, and hearing protective devices, as well as hearing loss prevention programs, risk factors, and information for specific industries and occupations






