


Tonsillopharyngitis is acute infection of the pharynx, palatine tonsils, or both. Symptoms may include sore throat, odynophagia, cervical lymphadenopathy, and fever. Diagnosis is clinical, supplemented by culture or rapid antigen test. Treatment depends on symptoms and, in the case of group A beta-hemolytic streptococcus, involves antibiotics.
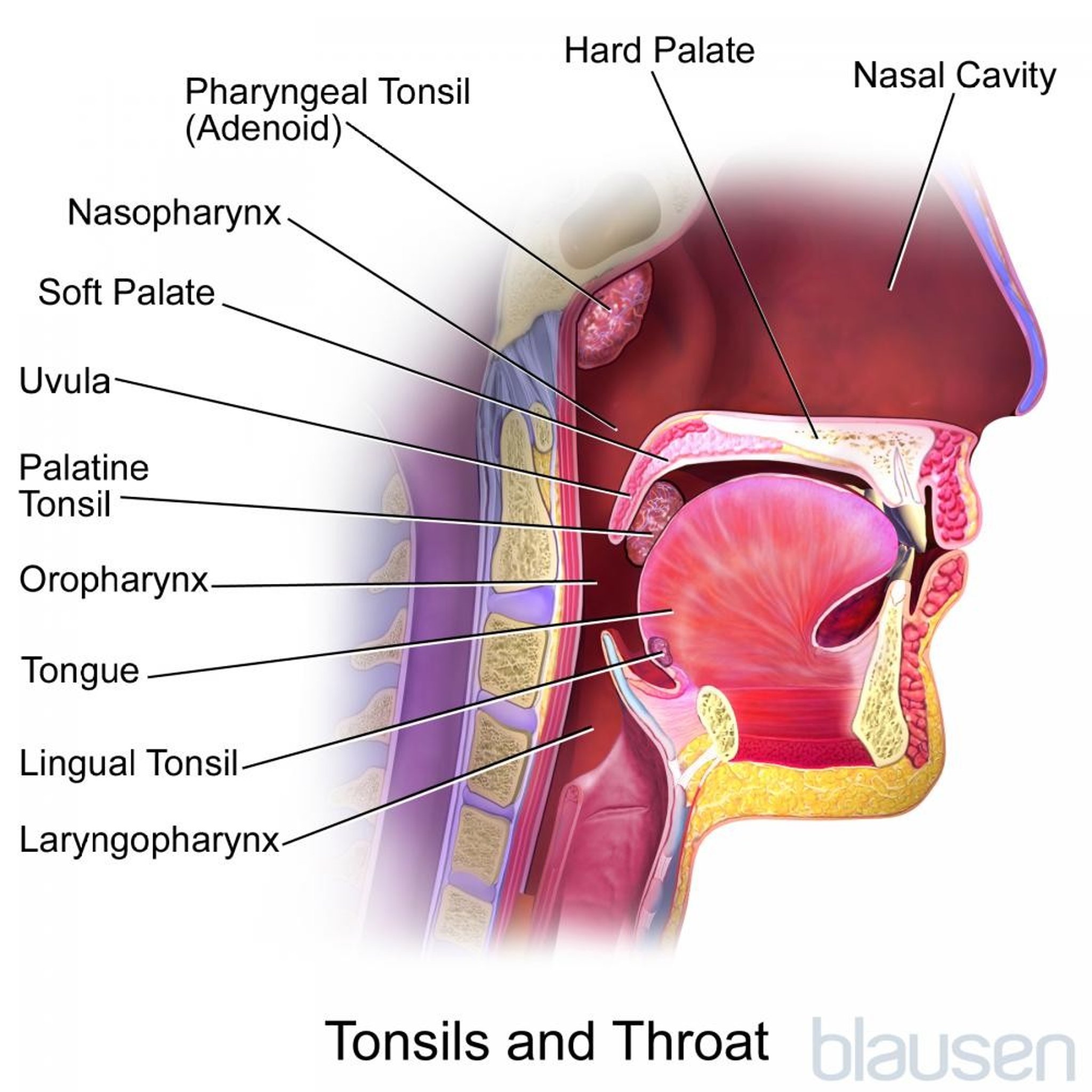
The tonsils participate in systemic immune surveillance. In addition, local tonsillar defenses include a lining of antigen-processing squamous epithelium that involves B- and T-cell responses.

Tonsillopharyngitis of all varieties is a very common cause of all office visits to primary care physicians.
(See also Streptococcal Infections.)
Etiology of Tonsillopharyngitis
Tonsillopharyngitis is usually viral, most often caused by the common cold viruses (adenovirus, rhinovirus, influenza, coronavirus, and respiratory syncytial virus), but occasionally by Epstein-Barr virus, herpes simplex virus, cytomegalovirus, or HIV.
In about 30% of patients, the cause is bacterial (1). Group A beta-hemolytic streptococcus (GABHS) is most common (see Streptococcal Infections), but Staphylococcus aureus, Streptococcus pneumoniae, Mycoplasma pneumoniae, and Chlamydia pneumoniae are sometimes involved. Rare causes include pertussis, Fusobacterium, diphtheria, syphilis, and gonorrhea.
GABHS occurs most commonly between ages 5 and 15 and is uncommon before age 3. It is less common among older adults.
Etiology reference
1. Pichichero ME: Group A streptococcal tonsillopharyngitis: cost-effective diagnosis and treatment. Ann Emerg Med 25 (3):390–403, 1995. doi: 10.1016/s0196-0644(95)70300-4
Symptoms and Signs of Tonsillopharyngitis
Pain when swallowing is the hallmark of tonsillopharyngitis and is often referred to the ears. Very young children who are not able to complain of sore throat often refuse to eat. High fever, malaise, headache, and GI upset are common, as are halitosis and a muffled voice. The tonsils are swollen and red and often have purulent exudates. Tender cervical lymphadenopathy may be present. Fever, adenopathy, palatal petechiae, and exudates are somewhat more common with GABHS than with viral tonsillopharyngitis, but there is much overlap; both tonsillopharyngitis and GABHS can cause petechiae. With GABHS, a scarlatiniform rash (scarlet fever) may be present.


Photo provided by Clarence T. Sasaki, MD.
GABHS usually resolves within 7 days, with or without antibiotics. Untreated GABHS may lead to local suppurative complications (eg, peritonsillar abscess or cellulitis) and sometimes leads to rheumatic fever or glomerulonephritis.
Diagnosis of Tonsillopharyngitis
Clinical evaluation
Group A beta-hemolytic streptococcus (GABHS) ruled out by rapid antigen test, culture, or both, routinely or selectively
Pharyngitis itself is easily recognized clinically. However, its cause is not. Rhinorrhea and cough usually indicate a viral cause. Infectious mononucleosis is suggested by posterior cervical or generalized adenopathy, hepatosplenomegaly, fatigue, and malaise for > 1 week; a full neck with petechiae of the soft palate; and thick tonsillar exudates. A dirty gray, thick, tough membrane that bleeds if peeled away indicates diphtheria (rare in the US).
Because GABHS requires antibiotics, it must be diagnosed early. Criteria for testing are controversial. Many authorities recommend testing with a rapid antigen test or culture for all children. Rapid antigen tests are specific but not sensitive and may need to be followed by a culture, which is about 90% specific and 90% sensitive. In adults, many authorities recommend using the following 4 criteria of the modified Centor score (1):
History of fever
Tonsillar exudates
Absence of cough
Tender anterior cervical lymphadenopathy
Patients who meet 1 or no criteria are unlikely to have GABHS and should not be tested. Patients who meet 2 criteria can be tested. Patients who meet 3 or 4 criteria can be tested or treated empirically for GABHS.
Diagnosis reference
1. Fine AM, Nizet V, Mandl KD: Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med 172 (11):847–852, 2012. doi: 10.1001/archinternmed.2012.950
Treatment of Tonsillopharyngitis
Symptomatic treatment
Antibiotics for GABHS
Tonsillectomy considered for recurrent GABHS
1). Corticosteroids are commonly used to treat tonsillopharyngitis because they can help relieve pain and increase consumption of food. Some clinicians do not use corticosteroids because of their adverse effects.
2); dose is 250 mg orally 2 times a day for 10 days for patients < 27 kg and 500 mg for those >≤
Treatment may be started immediately or delayed until culture results are known. If treatment is started presumptively, it should be stopped if cultures are negative. Follow-up throat cultures are not done routinely. They are useful in patients with multiple GABHS recurrences or if pharyngitis spreads to close contacts at home or school.
Tonsillectomy
Tonsillectomy has often been considered if GABHS tonsillitis recurs repeatedly (> 6 episodes/year, > 4 episodes/year for 2 years, or > 3 episodes/year for 3 years) or if acute infection is severe and persistent despite antibiotics. Other criteria for tonsillectomy include obstructive sleep apnea, recurrent peritonsillar abscess, and suspicion of cancer. (See also American Academy of Otolaryngology–Head and Neck Surgery Clinical Practice Guideline: Tonsillectomy in Children [Update].) Decisions should be individualized, based on patient age, multiple risk factors, and response to infection recurrences (3).
Numerous effective surgical techniques are used to perform tonsillectomy; they include electrocautery dissection, microdebrider, radiofrequency coblation, and sharp dissection. Postoperative IV rehydration is necessary in ≤ 3% of patients, possibly in fewer patients who have had optimal preoperative hydration, perioperative antibiotics, analgesics, and corticosteroids. Significant intraoperative or postoperative bleeding occurs in < 2% of patients, usually within 24 hours of surgery or after 7 days, when the eschar detaches. Patients with bleeding should go to the hospital. If bleeding continues on arrival, patients are usually examined in the operating room, and hemostasis is obtained. Any clot present in the tonsillar fossa is removed, and patients are observed for 24 hours.
Postoperative airway obstruction occurs most frequently in children < 2 years who have preexisting severe obstructive sleep disorders and in patients with morbid obesity or neurologic disorders, craniofacial anomalies, or significant preoperative obstructive sleep apnea. Complications are generally more common and serious among adults.
Accumulating evidence suggests that tonsillotomy (partial intracapsular removal of tonsil tissue), when done to treat various disorders is as efficacious as traditional tonsillectomy and preferable because of better outcomes related to pain, postoperative complications, and patient satisfaction (4, 5).
Treatment references
1. Hayward G, Thompson MJ, Perera R, et al: Corticosteroids as standalone or add-on treatment for sore throat. Cochrane Database Syst Rev., 2012. doi: 10.1002/14651858.CD008268.pub2
2. Shulman ST, Bisno AL, Clegg HW, et al: Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis 15;55 (10):e86-102, 2012. doi: 10.1093/cid/cis629 Epub 2012 Sep 9.
3. Ruben RJ: Randomized controlled studies and the treatment of middle-ear effusions and tonsillar pharyngitis: how random are the studies and what are their limitations? Otolaryngol Head Neck Surg. 139(3):333-9, 2008. doi: 10.1016
4. Wong Chung JERE, van Benthem PPG, Blom HM: Tonsillotomy versus tonsillectomy in adults suffering from tonsil-related afflictions: a systematic review. Acta Otolaryngol 138(5):492-501, 2018. doi: 10.1080/00016489.2017.1412500
5. Blackshaw H, Springford LR, Zhang L-Y, et al: Tonsillectomy versus tonsillotomy for obstructive sleep-disordered breathing in children. Cochrane Database Syst Rev 4 (4):CD011365, 2020. doi: 10.1002/14651858.CD011365.pub2
Key Points
Pharyngitis itself is easily recognized clinically; however, in 25 to 30% of cases, testing is likely to be required to determine whether the infection is a streptococcal infection (ie, strep throat).
Clinical criteria (modified Centor score) can help to select patients for further testing or empiric antibiotic treatment, although some authorities recommend testing all children using a rapid antigen test and sometimes culture.
Penicillin remains the drug of choice for streptococcal pharyngitis; cephalosporins or macrolides are alternatives for patients allergic to penicillin.






