


Diagnostic tests are indicated when the cause of a skin lesion or disease is not obvious from history and physical examination alone. These include
Examination by Wood light
(See also Evaluation of the Dermatologic Patient.)
Skin Biopsy
There are several types of skin biopsy:
Punch
Shave
Wedge excision
In a punch biopsy, a tubular punch (diameter usually 4 mm) is inserted into deep dermal or subcutaneous tissue to obtain a specimen, which is snipped off at its base.
Shaving
Wedge excision of skin using a scalpel can be done for larger or deeper biopsies, which are closed by sutures.
Pigmented lesions are sometimes excised for histologic evaluation of depth; if too superficial, definitive diagnosis may be impossible. Diagnosis and cure can often be achieved simultaneously for most small tumors by complete excision that includes a small border of normal skin.
Skin Scrapings
Skin scrapings help diagnose fungal infections and scabies.
For fungal infection, scale is taken from the border of the lesion and placed onto a microscope slide. Then a drop of 10 to 20% potassium hydroxide is added. Hyphae, budding yeast, or both confirm the diagnosis of tinea or candidiasis.
For scabies,
Wood Light
A Wood light (black light) can help clinicians diagnose and define the extent of lesions (eg, borders of pigmented lesions before excision). It can help distinguish hypopigmentation from depigmentation (depigmentation of vitiligo fluoresces ivory-white and hypopigmented lesions do not).
Erythrasma fluoresces a characteristic bright orange-red. Tinea capitis caused by Microsporum canis and M. audouinii fluoresces a light, bright green. (NOTE: Most tinea capitis in the United States is caused by Trichophyton species, which do not fluoresce.) The earliest clue to cutaneous Pseudomonas infection (eg, in burns) may be green fluorescence.


Tzanck Testing
Tzanck testing can be used to diagnose viral disease, such as herpes simplex and herpes zoster, and is done when active, intact vesicles are present. Tzanck testing cannot distinguish between herpes simplex and herpes zoster infections.
An intact blister is the preferred lesion for examination. The blister roof is removed with a sharp blade, and the base of the unroofed vesicle is scraped with a #15 scalpel blade. The scrapings are transferred to a slide and stained with Wright stain or Giemsa stain. Multinucleated giant cells are a sign of herpes infection.

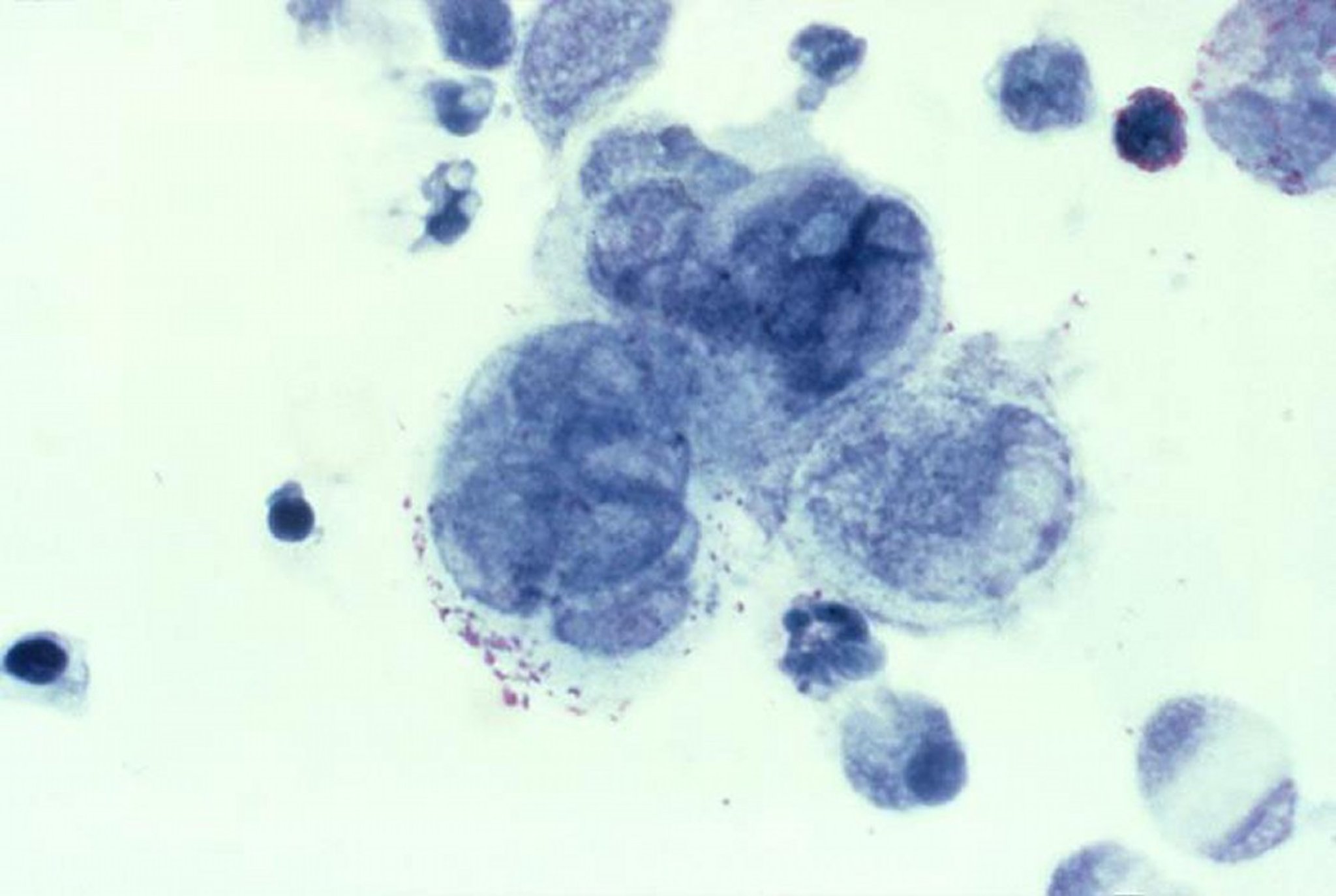
Photo courtesy of Joe Miller via the Public Health Image Library of the Centers for Disease Control and Prevention.
Diascopy
Diascopy is used to determine whether erythema in a lesion is due to blood within superficial vessels (inflammatory or vascular lesions) or is due to hemorrhage (petechiae or purpura).
A microscope slide is pressed against a lesion (diascopy) to see whether it blanches. Hemorrhagic lesions do not blanch; inflammatory and vascular lesions do.
Diascopy can also help identify sarcoid skin lesions, which, when tested, turn an apple jelly color.






