


Hemophilias are common hereditary bleeding disorders caused by deficiencies of either clotting factor VIII or IX. The extent of factor deficiency determines the probability and severity of bleeding. Bleeding into deep tissues or joints usually develops within hours of trauma. The diagnosis is suspected in a patient with an elevated partial thromboplastin time and normal prothrombin time and platelet count; it is confirmed by specific factor assays. Treatment includes replacement of the deficient factor if acute bleeding is suspected, confirmed, or likely to develop (eg, before surgery).
(See also Overview of Coagulation Disorders.)
Hemophilia A (factor VIII deficiency), which affects about 80% of patients with hemophilia, and hemophilia B (factor IX deficiency) have identical clinical manifestations and screening test abnormalities. Both are X-linked genetic disorders. Specific factor assays are required to distinguish the two.
Etiology of Hemophilia
Hemophilia is an inherited disorder that results from mutations, deletions, or inversions affecting the factor VIII or factor IX gene. Because these genes are located on the X chromosome, hemophilia affects males almost exclusively. Female children of males with hemophilia are obligate carriers, but male children are normal. Each male child of a carrier has a 50% chance of having hemophilia, and each female child has a 50% chance of being a carrier.
Some female carriers of hemophilia A or B become symptomatic during invasive procedures or childbirth. In these instances, the unaffected or normal X chromosome (with the normal factor VIII or IX gene) is preferentially inactivated. These females typically have factor levels in the same range as males with mild hemophilia (factor VIII or IX > 5% but < 50%). In patients undergoing surgery, the factor VIII or IX levels can be too low for normal hemostasis.
Pathophysiology of Hemophilia
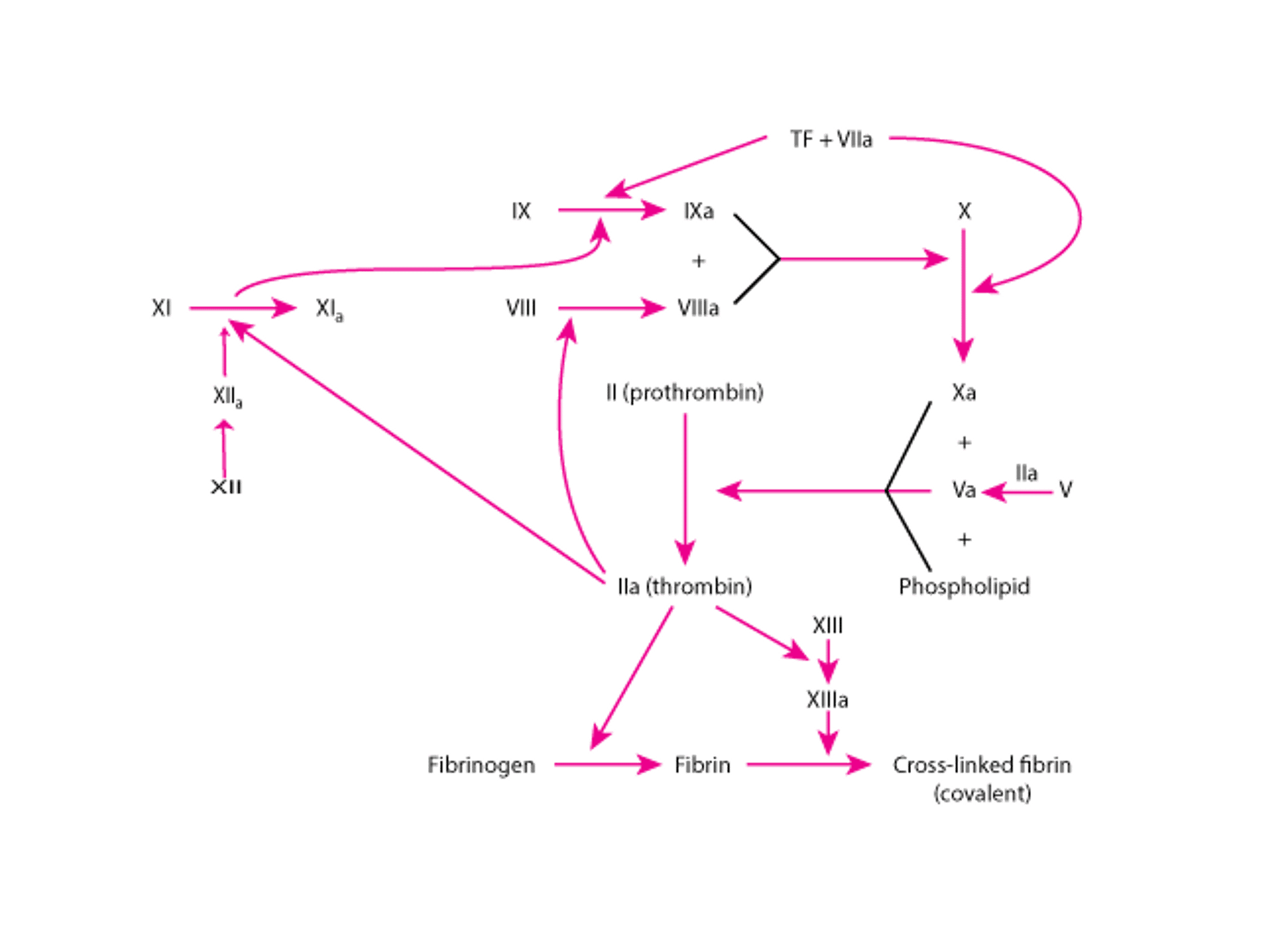
Normal hemostasis (see figure Pathways in Blood Coagulation) occurs when factor VIII and IX levels are ≥ 50% of normal. The gene abnormalities with severe hemophilia (factor levels < 1%) are typically large deletions or inversions or point mutations that disrupt gene expression. In contrast, hemophilia that is mild or moderate typically involves with point mutations that result in an amino acid change (missense mutation).
Sporadic cases of hemophilia A and B (where the female parent is not a carrier) are not unusual. In one study, 55% of patients with severe hemophilia A and 43% of patients with severe hemophilia B were sporadic cases. In mild and moderate hemophilia A and B, 30% of cases were sporadic (1).
Pathways in Blood Coagulation

Most patients with hemophilia who were treated in the early 1980s were infected with HIV, hepatitis B, or hepatitis C as a result of contaminated plasma or factor VIII or IX concentrates (before the development of effective viral inactivators). Occasional patients developed immune thrombocytopenia secondary to HIV infection, which exacerbates bleeding.
Pathophysiology reference
1. Kasper CK, Lin JC. Prevalence of sporadic and familial haemophilia. Haemophilia 2007;13(1):90-92. doi:10.1111/j.1365-2516.2006.01397.x
Symptoms and Signs of Hemophilia
Patients with hemophilia bleed into tissues (eg, hemarthroses, muscle hematomas, retroperitoneal hemorrhage). The bleeding may be immediate or occur slowly, depending on the extent of trauma and plasma level of factor VIII or IX. Pain often occurs as bleeding commences, sometimes before other signs of bleeding develop. Chronic or recurrent hemarthroses can lead to synovitis and arthropathy. Even a trivial blow to the head can cause intracranial bleeding. Bleeding into the base of the tongue can cause life-threatening airway compression.
In mild hemophilia (factor VIII or IX level 5 to 49% of normal), excessive bleeding may occur after surgery or dental extraction.
Moderate hemophilia (factor VIII or IX level 1 to 5% of normal) usually causes bleeding after minimal trauma.
Severe hemophilia (factor VIII or IX level < 1% of normal) causes severe bleeding throughout life, usually beginning soon after birth (eg, scalp hematoma after delivery or excessive bleeding after circumcision).
Diagnosis of Hemophilia
Platelet count, prothrombin time (PT), partial thromboplastin time (PTT), factor VIII and IX assays
Sometimes von Willebrand factor activity and antigen and multimer composition
Hemophilia is suspected in patients with recurrent bleeding, unexplained hemarthroses, or a prolongation of the PTT. If hemophilia is suspected, PTT, PT, platelet count, and factor VIII and IX assays are obtained. In hemophilia, the PTT is prolonged, but the PT and platelet count are normal.
Factor VIII and IX assays determine the type and severity of the hemophilia. Because factor VIII levels may also be reduced in von Willebrand disease, von Willebrand factor (VWF) activity, VWF antigen, and VWF multimer composition are measured in patients with newly diagnosed hemophilia A, particularly if the disorder is mild and a family history indicates that both male and female family members are affected. Determining if a female is a true carrier of hemophilia A is sometimes possible by measuring the factor VIII level. Similarly, measuring the factor IX level often identifies a carrier of hemophilia B. Definitive diagnosis requires genetic testing.
Polymerase chain reaction (PCR) analysis of DNA that comprises the factor VIII or factor IX gene, available at specialized centers, can be used for diagnosis of the hemophilia A or B carrier state and for prenatal diagnosis of hemophilia A or B by chorionic villus sampling at 12 weeks or amniocentesis at 16 weeks. These procedures carry a 0.5 to 1% risk of miscarriage. Studies of cell-free fetal DNA in maternal blood have shown promise as a noninvasive method to screen for hemophilia.
After repeated exposure to factor VIII or IX replacement, about 30% of patients with severe hemophilia A (1) and 3% with hemophilia B (2) develop (alloantibodies) that inhibit the coagulant activity of any additional factor VIII or factor IX infused. Thus, patients should be screened for isoantibodies (eg, by measuring the degree of PTT shortening immediately after mixing the patient’s plasma with an equal volume of normal plasma, and then by repeating the measurement after incubation for 1 hour), especially before an elective procedure that requires replacement therapy. If isoantibodies are present, their titers can be measured by determining the extent of factor VIII or factor IX inhibition by serial dilutions of patient plasma.
Pearls & Pitfalls
|
Diagnosis references
1. Iorio A, Fischer K, Makris M. Large scale studies assessing anti-factor VIII antibody development in previously untreated haemophilia A: what has been learned, what to believe and how to learn more. Br J Haematol 2017;178(1):20-31. doi:10.1111/bjh.14610
2. Puetz J, Soucie JM, Kempton CL, Monahan PE; Hemophilia Treatment Center Network (HTCN) Investigators. Prevalent inhibitors in haemophilia B subjects enrolled in the Universal Data Collection database. Haemophilia 2014;20(1):25-31. doi:10.1111/hae.12229
Treatment of Hemophilia
Replacement of the deficient factor
Sometimes antifibrinolytics
If symptoms suggest bleeding, treatment should begin immediately, even before diagnostic tests are completed. For example, treatment for headache that might indicate intracranial hemorrhage should begin before CT is completed.
Replacement of the deficient factor is the primary treatment.
In hemophilia A, the factor VIII trough level (ie, the factor VIII level measured immediately prior to the next dose) should be raised to
50% of normal to prevent bleeding after dental extraction or to abort an incipient joint hemorrhage
50 to 80% of normal for severe joint or intramuscular bleeding
100% of normal before major surgery or if bleeding is intracranial, intracardiac, or otherwise life threatening
Repeated infusions of the initial calculated dose should then be given every 8 to 12 hours to keep trough levels at 50 to 80% of normal for 7 to 14 days after major surgery or life-threatening hemorrhage. After neurosurgery or cardiac surgery, the factor trough level should be maintained at 100% of normal for the first 3 days after surgery. A trough level of 80 to 100% is targeted for postoperative days 4 to 7 followed by a target of 50 to 80% for postoperative days 8 to 14. After an intracranial bleed, the trough factor level should be maintained at 100% of normal for the first 7 days. The target should be 80 to 100% for days 8 to 14 and 50 to 80% for days 15 to 21. After an intracranial bleed, life-long factor prophylaxis is recommended. Each unit/kg of factor VIII increases the factor VIII level by about 2%. Thus, to increase the level from 0% to 50%, about 25 units/kg are required.
Factor VIII can be given as purified plasma-derived factor VIII concentrate, which is derived from multiple donors. It then undergoes viral inactivation, but inactivation may not eliminate parvovirus or hepatitis A virus. Recombinant factor VIII is free of viruses and is usually preferred.
In hemophilia B,factor IX is smaller than factor VIII and, in contrast to factor VIII, has an extensive extravascular distribution. Each unit/kg of factor IX increases the factor IX level by 1%. Due to extravascular distribution, the initial dose of factor IX is generally 25% higher than subsequent doses.
Fresh frozen plasma contains factor VIII and factor IX. However, unless plasma exchange is done, sufficient whole plasma usually cannot be given to patients with severe hemophilia to raise factor VIII or factor IX to levels that prevent or control bleeding. Fresh frozen plasma should, therefore, be used only if factor concentrates are not available.
Cryoprecipitate contains factor VIII and can be used as a replacement product if factor VIII concentrates are not available. Each unit of cryoprecipitate contains 80 units of factor VIII. Because plasma and cryoprecipitate are generally not virally inactivated, these blood products should be used only in emergencies when factor concentrates are not available.
A recombinant factor VIII-Fc fusion protein (1), a recombinant factor IX-Fc fusion protein (234) all have longer in vivo survival times and have been reported to control bleeding in hemophilia A and B.
factor IX and factor X and links them into a factor Xase-like active complex that obviates the need for factor VIII, is an effective treatment (5). Emicizumab is administered as a subcutaneous injection every 1, 2, or 4 weeks. It has a half-life of 28 days.
Therapeutic agents in clinical trials for both hemophilia A and B include fitusiran and concizumab (6, 7). Fitusiran is a small inhibitory RNA that knocks down the production of the natural anticoagulant protein, antithrombin. Concizumab is a humanized monoclonal antibody that blocks tissue factor pathway inhibitor (TFPI), another natural anticoagulant protein, and increases thrombin production in hemophilia A and B.
Gene therapy using adeno-associated virus (AAV) vectors has been shown in clinical trials to result in sustained factor VIII and factor IX expression (8, 9). An AAV vector gene therapy product for hemophilia B recently became available. An AAV vector gene therapy for hemophilia A is currently being evaluated (10).
Both VWF and factor VIII are stored in the Weibel-Palade bodies of endothelial cells and secreted in response to endothelial cell stimulation (11). Adjunctive therapy for mild hemophilia A may, therefore, include in vivo stimulation of patient endothelial cells with the synthetic vasopressin analogue DDAVP (deamino-D-argininevasopressinvon Willebrand disease, desmopressin may temporarily raise factor VIII levels. The patient’s response should be tested before desmopressin is used therapeutically. Its use after minor trauma or before elective dental surgery may obviate the need for replacement therapy. Desmopressin should be used only for patients with mild hemophilia A (basal factor VIII levels ≥ 5%) who have demonstrated responsiveness.
Treatment references
1. Mahlangu J, Powell JS, Ragni MV, et al: Phase 3 study of recombinant factor VIII Fc fusion protein in severe hemophilia A. Blood 123:317–325, 2014.
2. Powell JS, Pasi KJ, Ragni MV, et al: Phase 3 study of recombinant factor IX Fc fusion protein in hemophilia B. N Engl J Med 369:2313–2323, 2013.
3. Konkle BA, Stasyshyn O, Chowdary P, et al: Pegylated, full-length, recombinant factor VIII for prophylactic and on-demand treatment of severe hemophilia A. Blood 126:1078–1085, 2015.
4. Collins PW, Young G, Knobe K, et al. Recombinant long-acting glycoPEGylated factor IX in hemophilia B: A multinational randomized phase 3 trial. Blood 124:3880–3886, 2014.
5. Nuto A, Yoshihashi K, Takeda M, et al: Anti-factor IXa/X bispecific antibody (ACE910): Hemostatic potency against ongoing bleeds in a hemophilia A model and the possibility of routine supplementation. J Thromb Haemost 12:206–213, 2014.
6. Young G, Srivastava A, Kavakli K, et al. Efficacy and safety of fitusiran prophylaxis in people with haemophilia A or haemophilia B with inhibitors (ATLAS-INH): a multicentre, open-label, randomised phase 3 trial. Lancet 2023;401(10386):1427-1437. doi:10.1016/S0140-6736(23)00284-2
7. Shapiro AD, Angchaisuksiri P, Astermark J, et al. Subcutaneous concizumab prophylaxis in hemophilia A and hemophilia A/B with inhibitors: phase 2 trial results. Blood 2019;134(22):1973-1982. doi:10.1182/blood.2019001542
8. Perrin GQ, Herzog RW, Markusic DM. Update on clinical gene therapy for hemophilia. Blood 2019;133(5):407-414. doi:10.1182/blood-2018-07-820720
9. Samelson-Jones BJ, George LA. Adeno-Associated Virus Gene Therapy for Hemophilia. Annu Rev Med 2023;74:231-247. doi:10.1146/annurev-med-043021-033013
10. George LA: Hemophilia gene therapy comes of age. Blood Adv 1:2591–2599, 2017.
11. Turner NA and Moake JL: Factor VIII is synthesized in human endothelial cells, packaged in Weibel-Palade bodies and secreted bound to ULVWF strings. PLoS ONE 10(10): e0140740, 2015.
Prevention of Hemophilia
Family members who are carriers should be identified so that they may be offered genetic counseling.
To prevent bleeding, patients should avoid aspirin and nonsteroidal anti-inflammatory drugs (both inhibit platelet function). Regular dental care is essential so that tooth extractions and other dental surgery can be avoided. Medications should be given orally or IV; IM injections can cause hematomas.
Patients with hemophilia should be vaccinated against hepatitis A and hepatitis B.
Key Points
Hemophilias are X-linked recessive disorders of coagulation.
Patients bleed into tissues (eg, hemarthroses, muscle hematomas, retroperitoneal hemorrhage) following minimal trauma; fatal intracranial hemorrhage may occur.
The partial thromboplastin time is prolonged, but the prothrombin time and platelet count are normal; factor VIII and IX assays determine the type and severity of the hemophilia.
Patients with bleeding or in whom bleeding is anticipated (eg, before surgery or dental extraction) are given replacement factor, preferably using a recombinant product; dose depends on the circumstances.
About 30% of patients with severe hemophilia A who require repeated factor VIII infusions develop antibodies to factor VIII.






