


Legionella pneumophila
Legionella pneumophila was first recognized in 1976 after an outbreak at a convention of the American Legion in Philadelphia, Pennsylvania—thus, the name legionnaires’ disease. This disease is the pneumonic form of an infection usually caused by Legionella pneumophila serogroup 1. Nonpneumonic infection is called Pontiac fever, which manifests as a febrile, viral-like illness.
Transmission of Legionella species
Legionella organisms are often present in soil and fresh water. Amebas present in fresh water are a natural reservoir for these bacteria. Legionella organisms may enter a building's plumbing system via freshwater sources; a building’s water supply is often the source of a Legionella outbreak. Warm water temperatures of 25 to 40° C (77 to 104° F) support the highest concentrations of the organism in plumbing systems. Legionella organisms are embedded in a biofilm that forms on the inside of water pipes and containers. The infection is usually acquired by inhaling aerosols (or less often aspiration) of contaminated water (eg, as generated by shower heads, misters, decorative fountains, whirlpool baths, or water cooling towers for air-conditioning).
Legionella infection is not transmitted from person to person, although one probable case was reported in 2016 (1).
Transmission reference
1. Correia AM, Ferreira JS, Borges V, et al: Probable person-to-person transmission of Legionnaires' disease. N Engl J Med 374(5):497–498, 2016. doi: 10.1056/NEJMc1505356
Diseases caused by Legionella species
Legionella infection is more frequent and more severe in the following:
Older people
Patients with diabetes or chronic obstructive pulmonary disease (COPD)
Cigarette smokers
Immunocompromised patients (typically with diminished cell-mediated immunity)
The lungs are the most common site of infection; community- and hospital-acquired pneumonia may occur.
Extrapulmonary legionellosis is rare; manifestations include sinusitis, hip wound infection, myocarditis, pericarditis, and prosthetic valve endocarditis, frequently in the absence of pneumonia.
Symptoms and Signs of Legionella Infections
Legionnaires’ disease is a flu-like syndrome with acute fever, chills, malaise, myalgias, headache, or confusion. Nausea, loose stools or watery diarrhea, abdominal pain, cough, and arthralgias also frequently occur. Pneumonic manifestations may include dyspnea, pleuritic pain, and hemoptysis. Bradycardia relative to fever may occur, especially in severe cases.
Overall case fatality is low (about 5%) but can reach 40% in patients with hospital-acquired infections, older people, and immunocompromised patients.
Diagnosis of Legionella Infections
Direct fluorescent antibody staining
Sputum culture using specific growth media
Rapid urinary antigen test (for L. pneumophila serogroup 1 only)
Direct fluorescent antibody staining of sputum or bronchoalveolar lavage fluid is occasionally used but requires expertise. In addition, polymerase chain reaction testing with DNA probing is available and may help identify transmission pathways. A urinary antigen test is 60 to 95% sensitive and > 98% specific 3 days after symptom onset but detects only L. pneumophila (serogroup 1; 1), which accounts for 65% to 90% of cases (2, 3). Paired acute and convalescent antibody assays may yield a delayed diagnosis. A 4-fold increase or an acute titer of ≥ 1:128 is considered diagnostic.
Diagnosis of legionnaires' disease is by culture of sputum or bronchoalveolar lavage fluid; blood cultures are unreliable. Specific growth media are required. Slow growth on laboratory media may delay identification for 3 to 5 days.

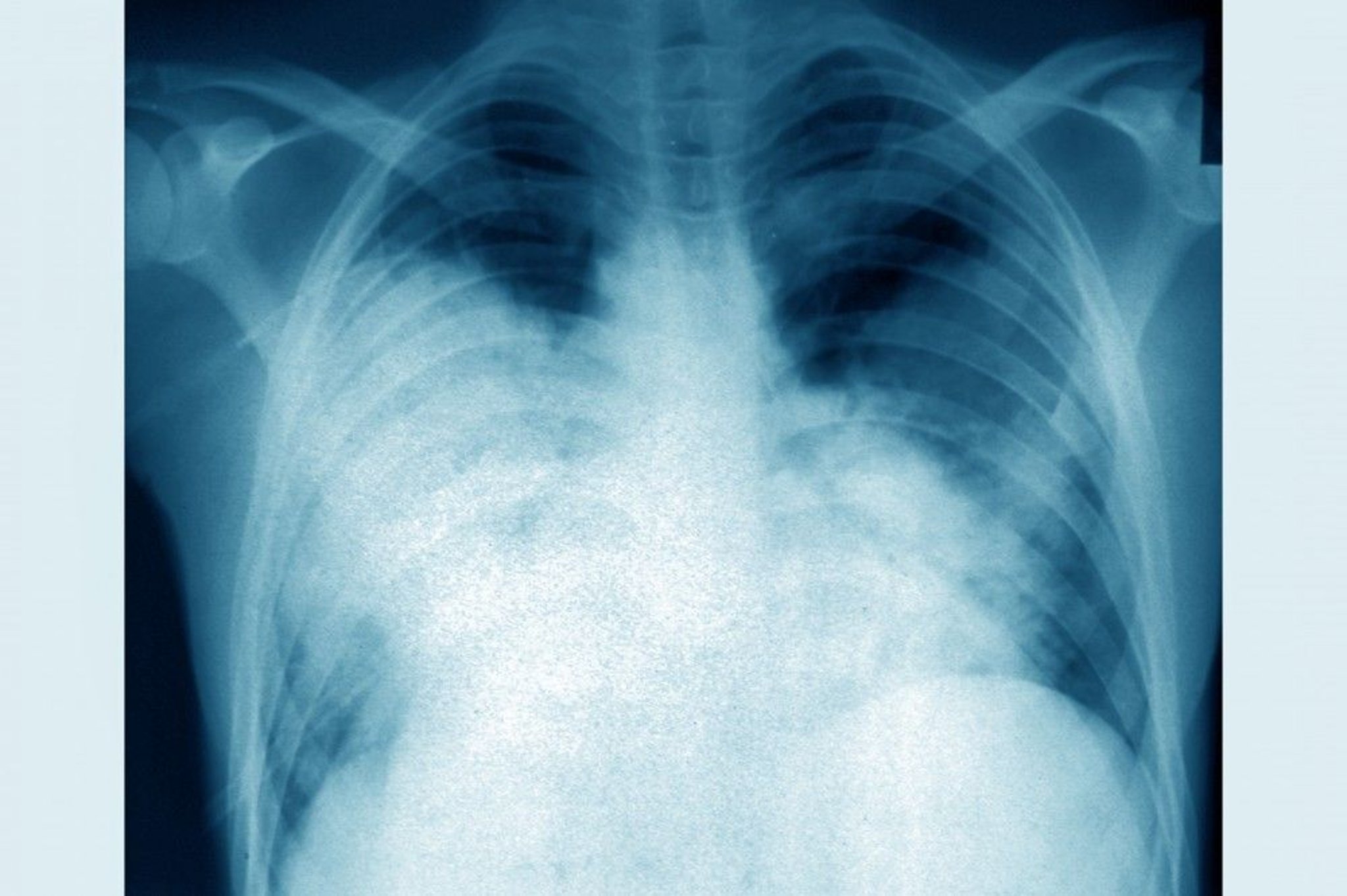
CAVALLINI JAMES/BSIP/SCIENCE PHOTO LIBRARY
Chest x-ray should be done; it usually shows patchy and rapidly asymmetrically progressive infiltrates (even when effective antibiotic therapy is used), with or without small pleural effusions.
Laboratory abnormalities often include hyponatremia, hypophosphatemia, and elevated aminotransferase levels and C-reactive protein.
Diagnosis references
1. Gassiep I, Armstrong M, Heather CS, Norton RE: Utility of the Legionella urinary antigen. Intern Med J 49(8):1050–1051, 2019. doi: 10.1111/imj.14381
2. Yu VL, Plouffe JF, Castellani Pastoris M, et al: Distribution of Legionella species and serogroups isolated by culture in patients with sporadic community-acquired legionellosis: An international collaborative survey. J Infect Dis 186(1):127–128, 2002. doi: 10.1086/341087
3. Avni T, Bieber A, Green H, et al: Diagnostic accuracy of PCR alone and compared to urinary antigen testing for detection of Legionella spp.: A systematic review. J Clin Microbiol 54(2):401–411, 2016. doi: 10.1128/JCM.02675-15
Treatment of Legionella Infections
Fluoroquinolones
Pontiac fever goes away on its own without treatment and causes no lingering problems.
Key Points
L. pneumophila usually causes pulmonary infection; it rarely causes extrapulmonary infections (most often involving the heart).
L. pneumophila infection is typically acquired by inhaling aerosols (or less often by aspiration) of contaminated water; it is not transmitted from person to person.
Diagnose using direct fluorescent antibody staining or polymerase chain reaction testing; sputum cultures are accurate but may take 3 to 5 days.
More Information
The following is an English-language resource that may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
Centers for Disease Control and Prevention (CDC): Legionella (Legionnaires' Disease and Pontiac Fever)






