


The complement system is an enzyme cascade that helps defend against infection via activation of a local inflammatory response. Many complement proteins occur in serum as inactive enzyme precursors (zymogens); others reside on cell surfaces. (See also Overview of the Immune System.)
The complement system bridges innate immunity and acquired immunity by
Augmenting antibody (Ab) responses and immunologic memory
Lysing foreign cells
Clearing immune complexes and apoptotic cells
Complement components have many biologic functions (eg, stimulation of chemotaxis, triggering of mast cell degranulation independent of immunoglobulin E [IgE]).
Complement activation
There are 3 pathways of complement activation (see figure Complement Activation Pathways):
Classical
Lectin
Alternative
Complement Activation Pathways
The classical, lectin, and alternative pathways converge into a final common pathway when C3 convertase (C3 con) cleaves C3 into C3a and C3b. Ab = antibody; Ag =antigen; C1-INH =C1 inhibitor; MAC = membrane attack complex; MASP = MBL-associated serine protease; MBL = mannose-binding lectin. Overbar indicates activation. |

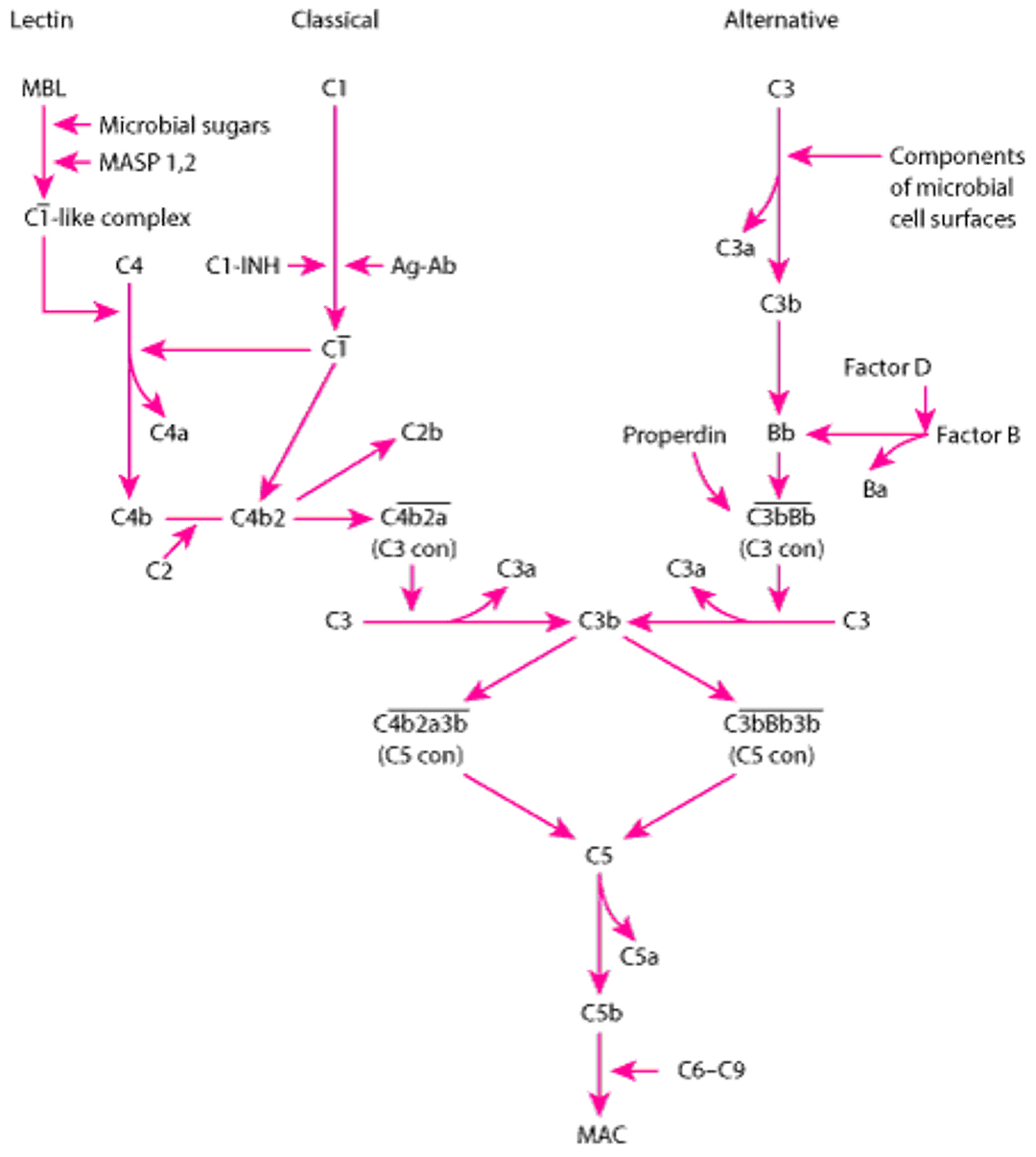
Classical pathway components are labeled with a C and a number (eg, C1, C3), based on the order in which they were identified. Alternative pathway components are often lettered (eg, factor B, factor D) or named (eg, properdin).
Classical pathway activation is either
Antibody-dependent, occurring when C1 interacts with antigen-IgM or aggregated antigen-IgG complexes
Antibody-independent, occurring when polyanions (eg, heparin, protamine, DNA and RNA from apoptotic cells), gram-negative bacteria, or bound C-reactive protein reacts directly with C1
This pathway is regulated by C1 inhibitor (C1-INH). Hereditary angioedema is due to a genetic deficiency of C1-INH.
Lectin pathway activation is antibody-independent; it occurs when mannose-binding lectin (MBL), a serum protein, binds to mannose, fucose, or N-acetylglucosamine groups on bacterial cell walls, yeast walls, or viruses. This pathway otherwise resembles the classical pathway structurally and functionally.
Alternate pathway activation occurs when components of microbial cell surfaces (eg, yeast walls, bacterial cell wall lipopolysaccharide [endotoxin]) or immunoglobulin (eg, nephritic factor, aggregated IgA) cleave small amounts of C3. This pathway is regulated by properdin, factor H, and decay-accelerating factor (CD55).
The 3 activation pathways converge into a final common pathway when C3 convertase cleaves C3 into C3a and C3b (see figure Complement Activation Pathways). C3 cleavage may result in formation of the membrane attack complex (MAC), the cytotoxic component of the complement system. MAC causes lysis of foreign cells.
Factor I, with cofactors including membrane cofactor protein (CD46), inactivates C3b and C4b.
Complement deficiencies and defects
Deficiencies or defects in specific complement components have been linked to specific disorders; the following are examples:
Deficiency in C1, C2, C3, MBL, MBL-associated serine protease 2 (MASP-2), factor H, factor I, or complement receptor 2 (CR2): Susceptibility to recurrent bacterial infections
Deficiency of C5, C9, factor B, factor D, or properdin: Susceptibility to neisserial infections
Defects in C1, C4, and C5: Systemic lupus erythematosus
Defects in CR2: Common variable immunodeficiency
Defects of CR3: Leukocyte adhesion deficiency type 1
Mutations in the genes for factor B, factor H, factor I, membrane cofactor protein (CD46), or C3: Development of the atypical variant of hemolytic uremic syndrome with microvascular thrombosis
Biologic activities of complement
Complement components have other immune functions that are mediated by complement receptors (CRs) on various cells. Several CRs use molecules that have been assigned a CD number.
CR1 (CD35) promotes phagocytosis and helps clear immune complexes.
CR2 (CD21) regulates antibody production by B cells and is the Epstein-Barr virus receptor.
CR3 (CD11b/CD18), CR4 (CD11c/CD18), and C1q receptors play a role in phagocytosis.
C3a, C5a, and C4a (weakly) have anaphylatoxin activity: They cause mast cell degranulation, leading to increased vascular permeability and smooth muscle contraction.
C3b acts as an opsonin by coating microorganisms and thereby enhancing their phagocytosis.
C3d enhances antibody production by B cells.
C5a is a neutrophil chemoattractant; it regulates neutrophil and monocyte activities and may cause augmented adherence of cells, degranulation and release of intracellular enzymes from granulocytes, production of toxic oxygen metabolites, and initiation of other cellular metabolic events.






