


Ascariasis is infection with Ascaris lumbricoides or occasionally Ascaris suum
(See also Approach to Parasitic Infections.)
Ascariasis, the most common intestinal helminth infection in the world, occurs worldwide but is concentrated in tropical and subtropical areas with poor sanitation. Prevalence is highest in children aged 2 to 10 years and decreases in older age groups. Current estimates suggest that about 500 million people are infected worldwide, and ascariasis contributes to malnutrition in areas with poor sanitation. It is estimated that ascariasis is responsible for 2,000 to 10,000 deaths worldwide annually, most of which are due to bowel or biliary tract obstruction in children.
In the United States, most cases occur in refugees, immigrants, or travelers to endemic tropical areas.
Humans are infected with A. lumbricoides when they ingest its eggs, often in food contaminated by human feces. Infection can also occur when hands or fingers with contaminated dirt on them are put in the mouth.
Humans can also be infected with ascaris (A. suum) from pigs when they ingest eggs from handling pigs or from consuming undercooked vegetables or fruits contaminated with pig feces. Whether A. suum is a distinct species from A. lumbricoides is debated.
Pathophysiology of Ascariasis
Ingested A. lumbricoides eggs hatch in the duodenum, and the resulting larvae penetrate the wall of the small bowel and migrate via the portal circulation through the liver to the heart and lungs. Larvae lodge in the alveolar capillaries, penetrate alveolar walls, and ascend the bronchial tree into the oropharynx. They are swallowed and return to the small bowel, where they develop into adult worms, which mate and release eggs into the stool. The life cycle is completed in about 2 to 3 months; adult worms live 1 to 2 years.

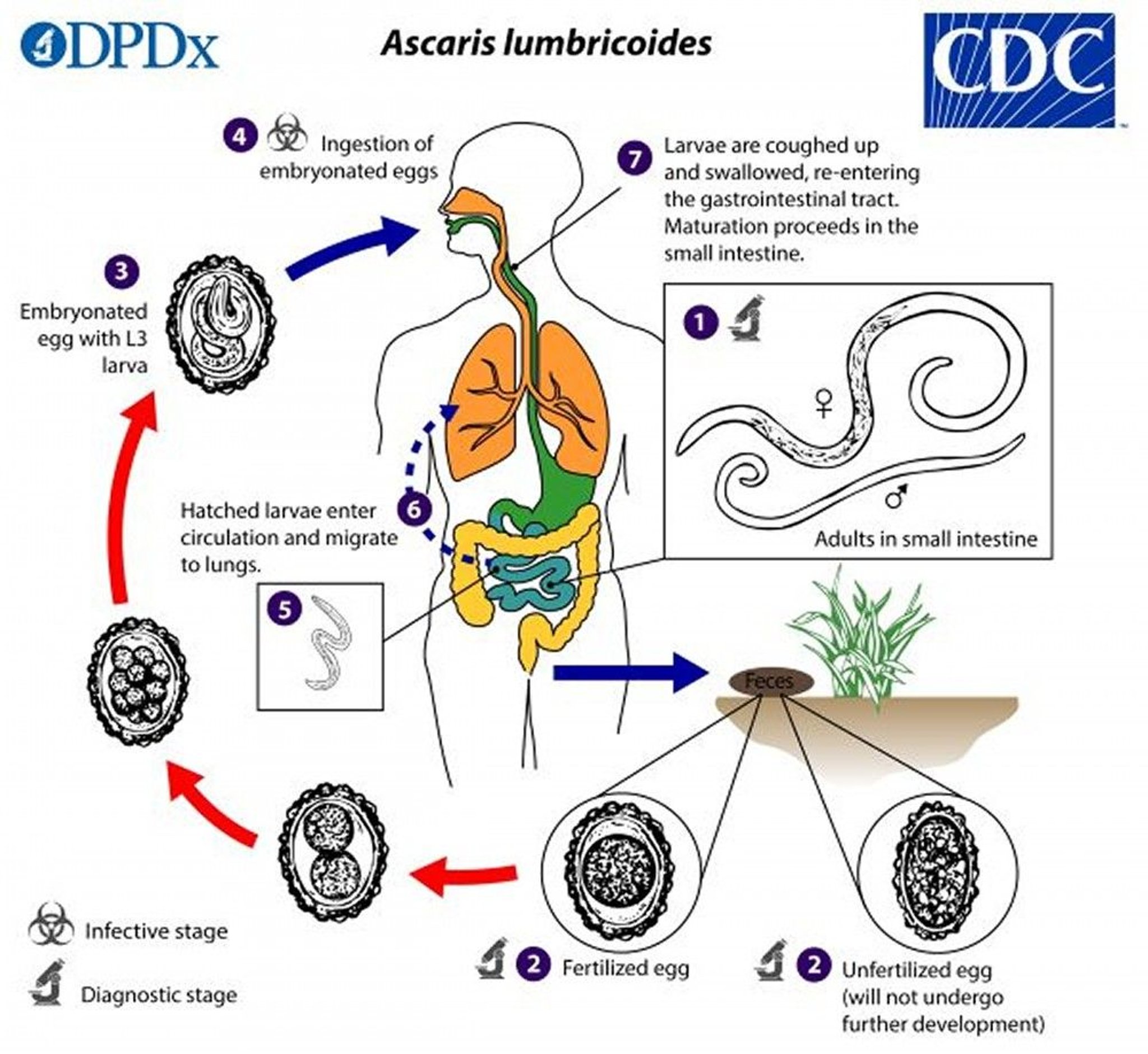
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Ascariasis
Ascaris larvae migrating through the lungs may cause cough, wheezing, and occasionally hemoptysis or other respiratory symptoms in people without prior exposure to Ascaris.
Adult worms in small numbers usually do not cause gastrointestinal symptoms, although passage of an adult worm by mouth or rectum may bring an otherwise asymptomatic patient to medical attention. Bowel or biliary obstruction causes cramping abdominal pain, nausea, and vomiting. Jaundice is uncommon.
Even moderate infections can lead to undernutrition in children. The pathophysiology is unclear and may include competition for nutrients, impairment of absorption, and depression of appetite.
Diagnosis of Ascariasis
Microscopic examination of stool
Identification of adult worms in stool or emerging from the nose, mouth, or rectum
Diagnosis of ascariasis is by microscopic detection of eggs in stool or observation of adult worms in stool or emerging from the nose or mouth. Occasionally, larvae can be found in sputum during the pulmonary phase. Adult worms may be seen in radiographic studies of the gastrointestinal tract.
Eosinophilia can be marked while larvae migrate though the lungs but usually subsides later when adult worms reside in the intestine. Chest x-ray during the pulmonary phase may show infiltrates, which in the presence of eosinophilia leads to the diagnosis of Löffler syndrome.
Treatment of Ascariasis
All intestinal Ascaris infections should be treated.
Albendazole, mebendazole, and ivermectin may harm the fetus, and risk of treatment in pregnant women infected with Ascaris must be balanced with risk of untreated disease. Before treatment with ivermectin, patients should be assessed for coinfection with Loa loa if they have lived in areas of central Africa where Loa loa
Ascaris infections but less effective for heavy infections. Piperazine, once widely used, has been replaced by less toxic alternatives.
Obstructive complications may be effectively treated with anthelmintic drugs or require surgical or endoscopic extraction of adult worms.
When the lungs are affected, treatment is symptomatic; it includes bronchodilators and corticosteroids. Anthelmintic drugs are typically not used.
Prevention of Ascariasis
Prevention of ascariasis requires adequate sanitation.
Preventive strategies include
Washing the hands thoroughly with soap and water before handling food
Washing, peeling, and/or cooking all raw vegetables and fruits before eating
Not eating uncooked or unwashed vegetables in areas where human or pig feces is used as fertilizer
Not defecating outdoors except in latrines with proper sewage disposal
Key Points
Ascariasis is the most prevalent intestinal helminth infection in the world.
Eggs hatch in the intestines, and larvae migrate first to the lungs and then to the intestines, where they mature.
Larvae in the lungs may cause cough and wheezing; masses of adult worms may obstruct the intestines and single adult worms may migrate into and obstruct bile or pancreatic ducts.
Diagnose by microscopic examination of the stool; occasionally, adult worms are seen.






