


Dracunculiasis is infection with Dracunculus medinensis. Symptoms are a painful, inflamed skin lesion, which contains an adult worm, and debilitating arthritis. Diagnosis is by inspection. Treatment is slow removal of the adult worm. Dracunculiasis is close to being eradicated.
(See also Approach to Parasitic Infections.)
In the mid-1980s, 3.5 million people had dracunculiasis, but by 2018, due to international efforts to interrupt transmission, only 28 cases were reported. In 2021, only 14 cases were reported in humans (1). Transmission remains within a narrow belt of African countries—Chad, Mali, Ethiopia, and possibly Sudan and South Sudan.
The guinea worm is likely to be the first human parasite to be eradicated (2).
General references
Pathophysiology of Dracunculiasis
Humans become infected by drinking water containing infected microcrustaceans (copepods). The larvae are released, penetrate the bowel wall, and mature in the abdominal cavity into adult worms in about 1 year.
After mating, the male dies, and the gravid female migrates through subcutaneous tissues, usually to the distal lower extremities. The cephalic end of the worm produces an indurated papule that vesiculates and eventually ulcerates. On contact with water (eg, when a person attempts to relieve the severe discomfort by immersing the affected limb), a loop of the worm’s uterus prolapses through the skin and discharges motile larvae. Worms that do not reach the skin die and disintegrate or become calcified. Larvae are ingested by copepods.
In most endemic areas, transmission is seasonal and each infectious episode lasts about 1 year.

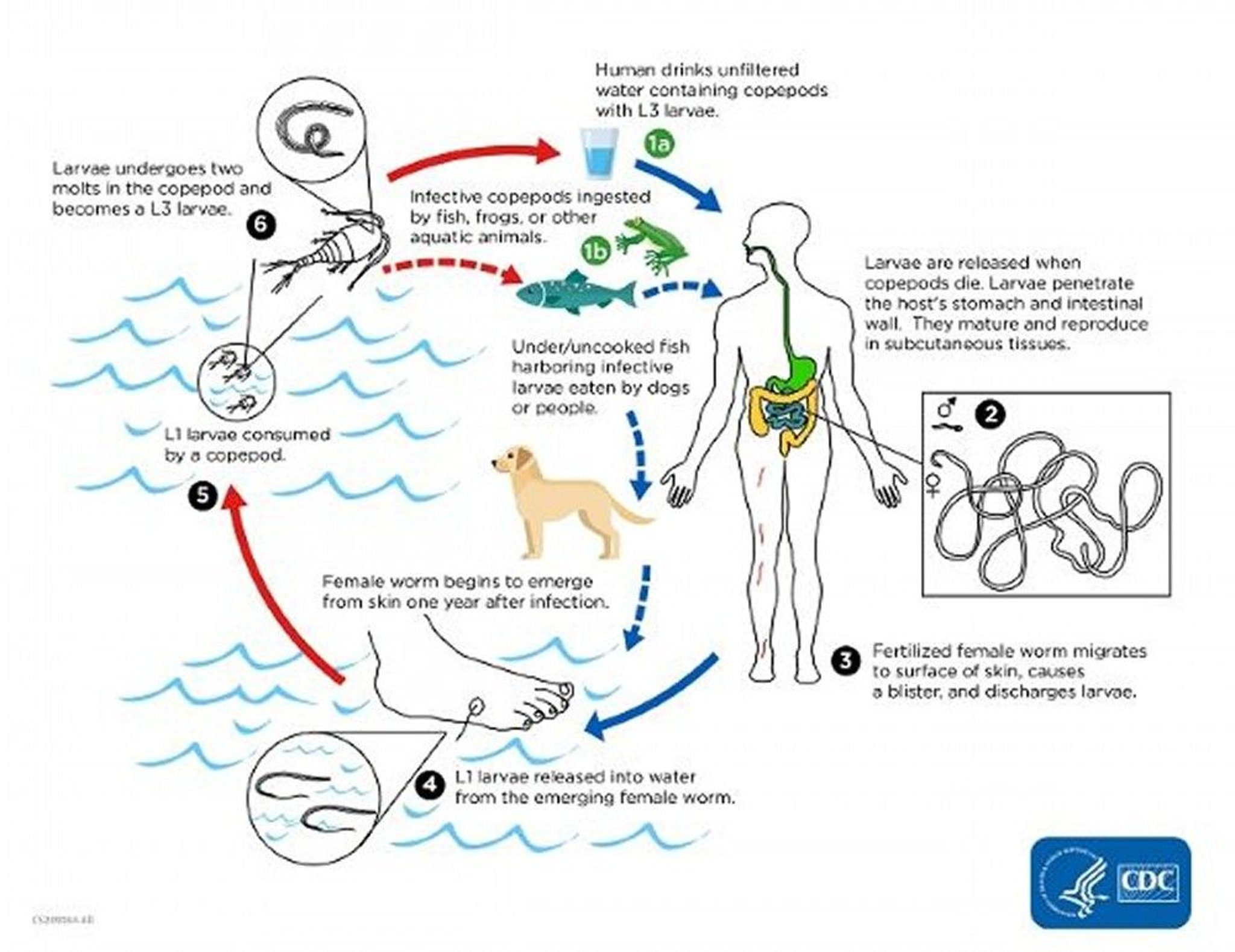
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Dracunculiasis
Dracunculiasis is typically asymptomatic for the first year. Symptoms develop when the worm erupts through the skin. Local symptoms include intense itching and a burning pain at the site of the skin lesion. Urticaria, erythema, dyspnea, vomiting, and pruritus are thought to reflect allergic reactions to worm antigens. If the worm is broken during expulsion or extraction, a severe inflammatory reaction ensues, causing disabling pain. Symptoms subside and the ulcer heals once the adult worm is expelled. In about 50% of cases, secondary bacterial infections occur along the track of the emerging worm.
The chronic stage of infection is associated with inflammation and pain in the joints and other signs of arthritis. Sequelae include fibrous ankylosis of joints and contraction of tendons.
Diagnosis of Dracunculiasis
Clinical evaluation
Diagnosis of dracunculiasis is obvious once the white, filamentous adult worm appears at the cutaneous ulcer. Calcified worms can be localized with x-ray examination; they have been found in Egyptian mummies.
No serodiagnostic tests are available.
Treatment of Dracunculiasis
Manual removal
Treatment of dracunculiasis consists of slow removal of the adult worm (which may be up to 80 cm long) over days to weeks by rolling it on a stick. Surgical removal under local anesthesia is an option but is seldom available in endemic areas.
Prevention of Dracunculiasis
Filtering drinking water through a piece of fine-mesh cloth, chlorination, or boiling effectively protects against dracunculiasis. Infected people should be instructed not to enter drinking water sources to avoid contaminating them. Improving access to clean water is an important public health measure.
Key Points
The guinea worm has almost been eradicated.
When an infected person immerses the affected extremity in water to relieve the intense discomfort caused by eruption of the female worm through the skin, larvae are released and ingested by microcrustaceans; humans are infected when they ingest water contaminated with the microcrustaceans.
If a worm is broken during expulsion or extraction, a severe inflammatory reaction ensues, causing disabling pain.
Diagnose based on observation of a white, filamentous adult worm at a cutaneous ulcer.
Treat dracunculiasis by slowly removing the adult worm over days to weeks by rolling it on a stick or sometimes by surgically removing it.
Filtering drinking water through a piece of fine-mesh cloth, chlorination, or boiling effectively protects against dracunculiasis.






