


Echinococcosis is infection with larvae of the tapeworm Echinococcus granulosus (cystic echinococcosis, hydatid disease) or Echinococcus multilocularis
Echinococcus granulosus is common in sheep-raising areas of the Mediterranean, Middle East, Australia, New Zealand, South Africa, and South America. Foci also exist in regions of Canada, Alaska, and California. Dogs are the definitive hosts, which may have adult tapeworms in their gastrointestinal tract, and herbivores (eg, sheep, goats, swine, cattle, camels, horses, deer) or humans are intermediate hosts that develop cystic lesions in the liver or other organs.
Adult E. multilocularis worms are present in foxes, coyotes, and dogs, and the hydatid larvae occur in small wild rodents. Infected dogs are the primary link to occasional human infection. E. multilocularis occurs mainly in Central Europe, Alaska, Canada, and Siberia. Its range of natural infection in the continental United States extends from Wyoming and the Dakotas to the upper Midwest.
Rarely, Echinococcus vogelii or Echinococcus oliganthus causes hydatid disease in humans, primarily in the liver. The disease may be polycystic (E. vogelii) or unicystic (E. oliganthus). These species occur in Central and South America.
Pathophysiology of Echinococcosis
Ingested eggs from animal feces (which may be present on the fur of dogs or other animals) hatch in the gut and release oncospheres (immature forms of the parasite enclosed in an embryonic envelope). Oncospheres penetrate the intestinal wall, migrate via the circulation, and lodge in the liver or lungs or, less frequently, in the brain, bone, or other organs. No adult worms are present in the gastrointestinal tract of humans.
In tissue, E. granulosus oncospheres develop into cysts, which grow slowly (usually over many years) into large unilocular, fluid-filled lesions—hydatid cysts. Brood capsules containing numerous small infective protoscolices form within these cysts. Large cysts may contain > 1 L of highly antigenic hydatid fluid as well as millions of protoscolices. Daughter cysts sometimes form in or outside primary cysts. If a cyst in the liver leaks or ruptures, infection can spread to the peritoneum.

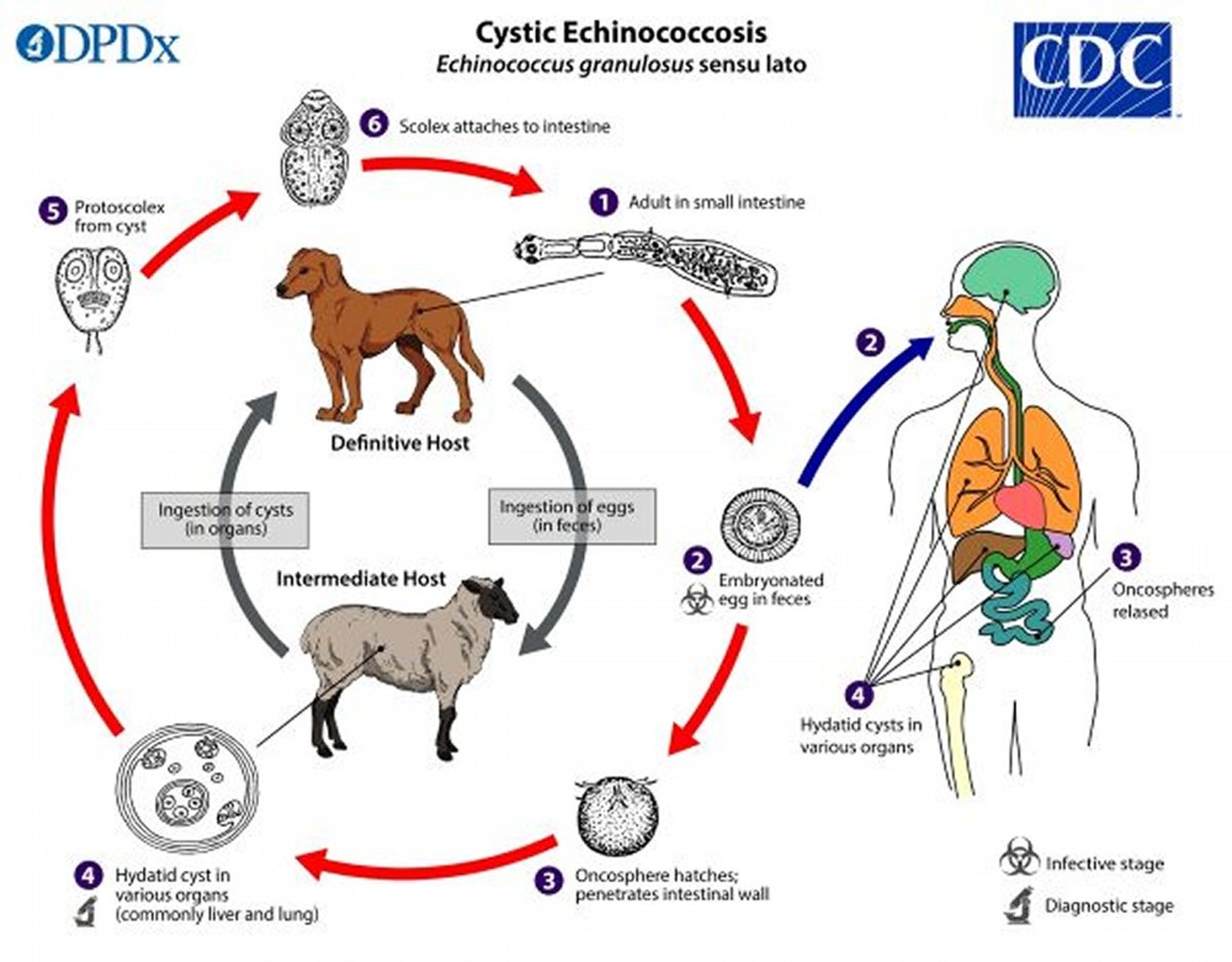
Image from the Centers for Disease Control and Prevention Image Library, Global Health, Division of Parasitic Diseases and Malaria.
E. multilocularis produces spongy masses that are locally invasive and difficult or impossible to treat surgically. Cysts occur primarily in the liver but can occur in the lungs, or other tissues. The cysts are not large, but they invade and destroy surrounding tissue and can cause liver failure and death.
Symptoms and Signs of Echinococcosis
Although many infections are acquired during childhood, clinical signs of echinococcosis may not appear for years, except when cysts are in vital organs. Symptoms and signs may resemble those of a space-occupying tumor.
Liver cysts may eventually cause abdominal pain or a palpable mass. Jaundice may occur if the bile duct is obstructed. Rupture into the bile duct, peritoneal cavity, or lung may cause fever, urticaria, or a serious anaphylactic reaction.
Pulmonary cysts can rupture, causing cough, chest pain, and hemoptysis.
Diagnosis of Echinococcosis
Imaging
Serologic testing
Examination of cyst fluid
CT, MRI, and ultrasound findings of the abdomen can be pathognomonic for cystic echinococcosis in the liver if daughter cysts and hydatid sand (protoscolices and debris) are present, but simple hydatid cysts may be difficult to differentiate from benign cysts, abscesses, or benign or malignant tumors. The presence of hydatid sand (scolices pass into the cyst fluid and form a white sediment) in aspirated cyst fluid is diagnostic. World Health Organization criteria use imaging results to categorize cysts as active, transitional, or inactive (1). Pulmonary involvement may present as round or irregular pulmonary masses on chest x-ray. Alveolar echinococcosis typically presents as an invasive mass.
Serologic tests (enzyme immunoassay, indirect hemagglutination assay) are sensitive in detecting infection., which can be confirmed by demonstrating echinococcal antigens using immunodiffusion (arc 5) or immunoblot assays. Complete blood count may detect eosinophilia.
Treatment of Echinococcosis
For hepatic echinococcosis, surgical resection
Percutaneous aspiration followed by instillation of a scolicidal agent and reaspiration (PAIR)
Observation only
Treatment of cystic (hydatid) echinococcosis varies depending on the type, location, and number of cysts and whether imaging results indicate the cysts are active, transitional, or inactive (1).
2).
Observation only is an option for asymptomatic cysts that are naturally inactivated (not inactivated by drug treatment).
Liver transplantation has been lifesaving in a few patients.
Pearls & Pitfalls
|
Patients with alveolar echinococcosis due to E. multilocularis
Treatment references
1. Nabarro LE, Amin Z, Chiodini PL: Current management of cystic echinococcosis: a survey of specialist practice. Clin Infect Dis. 60(5):721-8, 2015. doi: 10.1093/cid/ciu931.
2. Bildik N, Cevik A, Altintaş M, Ekinci H, Canberk M, Gülmen MJ Clin Gastroenterol 41(3):312-316, 2007. doi:10.1097/01.mcg.0000225572.50514.e6
3. Horton RJActa Trop64(1-2):79-93, 1997. doi:10.1016/s0001-706x(96)00640-7
Key Points
Echinococcosis occurs when ingested tapeworm eggs hatch, releasing oncospheres, which migrate into the liver or lungs or, less frequently, to the brain, bone, or other organs and develop into cysts; no adult worms are present in the gastrointestinal tract of humans.
The cysts of E. granulosus develop slowly (usually over many years) into large (up to 1 L), fluid-filled cysts (hydatid cysts), which contain numerous infective protoscolices.
Feces from infected dogs (and other canines) are the main source of human infection.
Liver cysts cause pain and sometimes jaundice; lung cysts can cause pain, cough, and hemoptysis.
E. multilocularis does not produce large cysts but invades and destroys surrounding tissue and can result in liver failure and death.
Diagnose by CT, MRI, or ultrasound, analysis of cyst fluid, and serologic testing.
Treatment varies depending on the infecting Echinococcus






