


Human African trypanosomiasis is infection with protozoa of the species Trypanosoma brucei
Human African trypanosomiasis is caused by Trypanosoma brucei gambiense in West and Central Africa and by T. brucei rhodesiense in East Africa; both species are endemic in Uganda. Trypanosoma brucei gambiense accounts for 98% of all cases of African trypanosomiasis, and T. brucei rhodesiense accounts for 2%. African trypanosomiasis has been targeted for eradication by the World Health Organization (WHO) and, as a result of control efforts, there has been a dramatic decrease (> 95%) in the number of reported cases worldwide. In 2021, approximately 800 combined cases were reported to the WHO, with over 90% caused by T. b. gambiense (see WHO: Human African trypanosomiasis). On average, 1 case is diagnosed in the US each year, always in travelers returning to the US from endemic regions.
The organisms are transmitted by tsetse flies and can be transmitted prenatally from mother to fetus. Rarely, the infection is transmitted through blood transfusions; theoretically, it could be transmitted through organ transplantation.
Another trypanosomal species, Trypanosoma cruzi, is endemic in South and Central America and causes Chagas disease (American trypanosomiasis).
Pathophysiology of African Trypanosomiasis
Metacyclic trypomastigotes inoculated by tsetse flies transform into bloodstream trypomastigotes, which multiply by binary fission and spread through the lymphatics and bloodstream after inoculation. Bloodstream trypomastigotes multiply until specific antibodies produced by the host sharply reduce parasite levels. However, a subset of parasites escape immune destruction by a change in their variant surface glycoprotein and start a new multiplication cycle. The cycle of multiplication and lysis repeats.
Late in the course of African trypanosomiasis, trypanosomes appear in the interstitial fluid of many organs, including the myocardium and eventually the central nervous system. The cycle is continued when a tsetse fly bites an infected human or animal.
Humans are the main reservoir of T. b. gambiense, but this species may also reside in animals. Wild game animals are the main reservoir of T. b. rhodesiense.

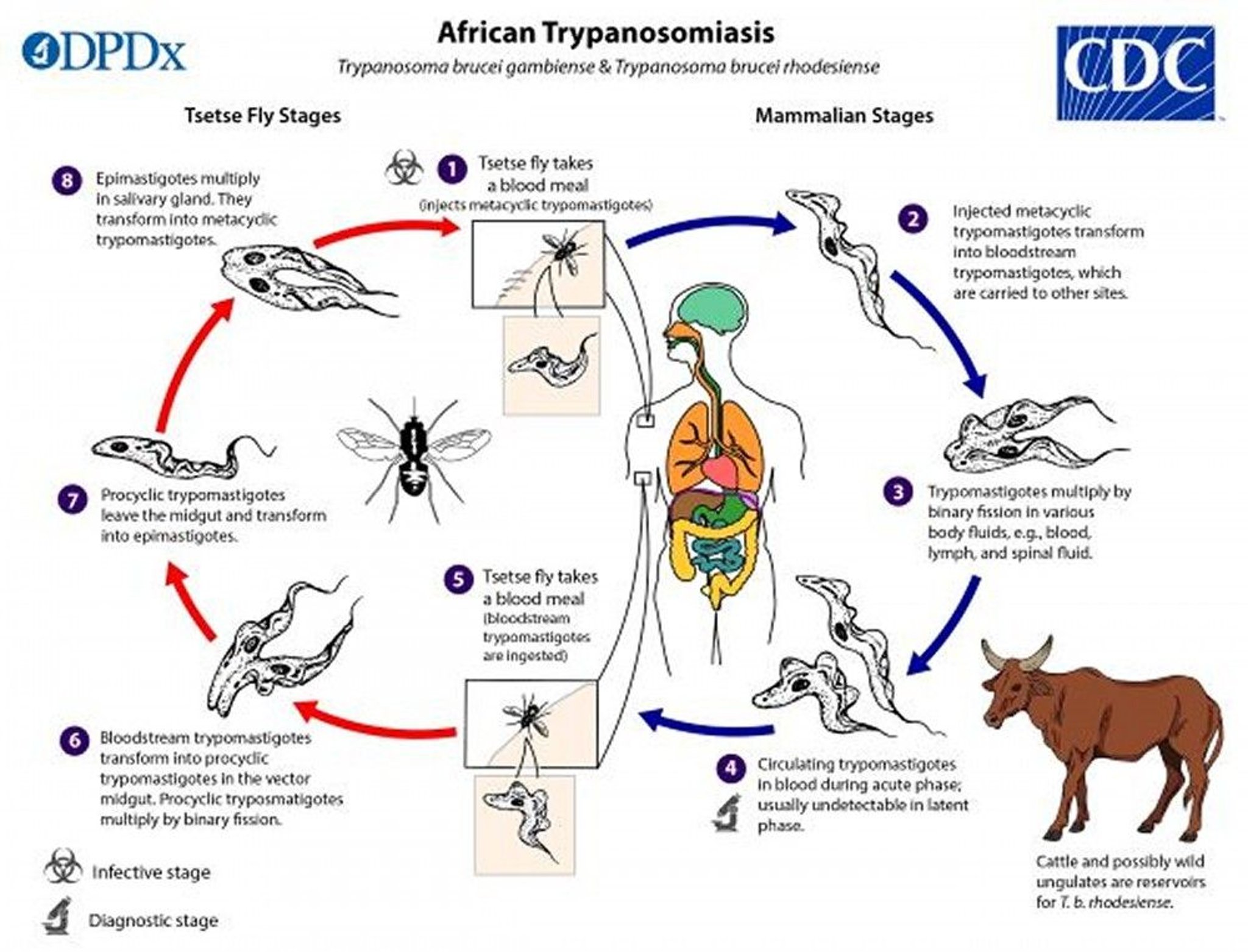
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of African Trypanosomiasis
African trypanosomiasis has 3 stages:
Cutaneous
Hemolymphatic
Central nervous system
Cutaneous
A papule may develop at the site of the tsetse fly bite within a few days to 2 weeks. It evolves into a red, painful, indurated nodule that may ulcerate (trypanosomal chancre).
Hemolymphatic
Over several months in T. b. gambiense infection but a period of weeks with T. b. rhodesiense, intermittent fever, headaches, rigors, muscle and joint pain, and transient facial swelling develop. An evanescent, circinate erythematous rash may develop. It is most readily visible in light-skinned patients. Generalized lymphadenopathy often occurs.
Winterbottom sign (enlarged lymph nodes in the posterior cervical triangle) is characteristic with T. b. gambiense sleeping sickness.
Central nervous system (CNS)
In the Gambian form, CNS involvement occurs months to several years after onset of acute disease. In the Rhodesian form, disease is more fulminant, and CNS invasion often occurs within a few weeks.
CNS involvement can result in persistent headache, inability to concentrate, personality changes (eg, progressive lassitude and indifference), daytime somnolence, tremor, ataxia, and terminal coma.
Without treatment, death occurs within months of disease onset with T. b. rhodesiense and during the 2nd or 3rd year with T. b. gambiense. Untreated patients die in coma of undernutrition or secondary infections.
Diagnosis of African Trypanosomiasis
Light microscopy of blood (thin or thick smears) or other fluid sample
Diagnosis of African trypanosomiasis is made by identifying trypanosomes in fluid from a chancre, lymph node aspirate, blood, bone marrow aspirate, or, during the late stage of infection, cerebrospinal fluid (CSF). Preferred sources are blood smears for T. b. rhodesiense and fluid aspirated from an enlarged lymph node for T. b. gambiense. Wet preparations should be examined for motile trypanosomes, and smears should be fixed, stained with Giemsa (or Field) stain, and examined. The concentration of trypanosomes in blood is often low, and concentration techniques (eg, centrifugation, miniature anion-exchange centrifugation, quantitative buffy coat technique) enhance sensitivity.
Antibody detection assays are not very useful clinically because seroconversion occurs after the onset of symptoms. However, a card agglutination test for T. b. gambiense is useful in mass screening programs to identify candidates for microscopic examination.
A lumbar puncture should be done in all patients with African trypanosomiasis. When CSF is involved, opening pressure may be increased, and CSF has elevated levels of lymphocytes (≥ 6 cells/mcL), total protein, and nonspecific IgM. In addition to trypanosomes, characteristic Mott cells (plasma cells with cytoplasmic vacuoles that contain immunoglobulin [Russell bodies]) may be present.
Other, nonspecific laboratory findings include anemia, monocytosis, and markedly elevated serum levels of polyclonal IgM.
Treatment of African Trypanosomiasis
Treatment of African trypanosomiasis is guided by species and stage of disease.
T. b. gambiense; suramin for T. b. rhodesiense
T. b. gambienseeflornithine is not available), for severe T. b. gambiense; melarsoprol for T. b. rhodesiense
T. b. gambiense, with or without CNS involvement. (See the World Health Organization
For patients ≥ 35 kg: 1800 mg/day in the loading phase (4 days), followed by 1200 mg/day in the maintenance phase (6 days)
For patients 20 to 34 kg: 1200 mg/day in the loading phase (4 days), followed by 600 mg/day in the maintenance phase (6 days)
Criteria for inpatient treatment includes any of the following characteristics:
Body weight < 35 kg
At risk for poor compliance
History of psychiatric disorders (to monitor for neuropsychiatric reactions)
Without central nervous system (CNS) involvement
T. b. gambiense without CNS involvement.
T. brucei subspecies but do not cross the blood-brain barrier and are not useful for CNS infection.
Pentamidine is used for T. b. gambiense
Suramin is the only drug effective for the hemolymphatic stage of T. b. rhodesiense. Suramin is not used to treat T. b. gambiense, because although potentially effective, it has been associated with adverse effects, including nausea, vomiting, photophobia, hyperesthesias, peripheral neuropathy, nephrotoxicity, urticaria, and pruritus. Also, serious hypersensitivity reactions can occur in patients co-infected with Onchocerca volvulus, which is endemic in many areas of West Africa where T. b. gambiense occurs.
The dosage of pentamidine is 4 mg/kg IM or IV once a day for 7 to 10 days.
An initial test dose of suramin (available from the Centers for Disease Control and Prevention [CDC]) 100 mg IV (to exclude hypersensitivity) is followed by 20 mg/kg (up to 1 g) IV on days 1, 3, 7, 14, and 21.
With central nervous system (CNS) involvement
T. b. gambiense.
T. b. gambiense (eflornithine is ineffective for T. b. rhodesiense). WHO recommends eflornithine1eflornithine
Melarsoprol, an organic arsenical, is often used in African countries because of the limited availability of eflornithine, even though adverse effects can be severe and life threatening. Melarsoprol dosage is as follows:
For T. b. gambiense: 2.2 mg/kg (maximum dose 180 mg) IV once a day for 10 days
For T. b. rhodesiense: 2 to 3.6 mg/kg IV once a day for 3 days; after 7 days, 3.6 mg/kg once a day for 3 days, followed 7 days later by another 3-day course at this dose
In the US, eflornithine
Alternative regimens have been proposed for debilitated patients with severe CNS involvement. Serial follow-up examinations, including cerebrospinal fluid analysis, are recommended every 6 months (sooner if symptoms return) for 2 years.
Serious adverse effects of melarsoprol include encephalopathic reactions, exfoliative dermatitis, cardiovascular toxicity (hypertension, arrhythmia, heart failure), and the gastrointestinal and renal toxicity of arsenicals.
Corticosteroids have been used to decrease the risk of encephalopathic reactions.
There is no test of cure. After treatment, patients should be monitored for relapse for 24 months. Recurrence of symptoms necessitates re-examination of CSF for parasites.
Treatment reference
1. World Health Organization: WHO publishes new guidelines for the treatment of sleeping sickness; August 2019.
Prevention of African Trypanosomiasis
Prevention of African trypanosomiasis includes avoiding endemic areas and protecting against tsetse flies.
Visitors to game parks should wear substantial wrist- and ankle-length clothing (tsetse flies bite through thin clothes) in neutral colors that blend with the background and should use insect repellents, although efficacy of repellents against tsetse flies may be limited.
T. b. gambiense infection, but it may damage pancreatic beta cells, resulting in insulin release and hypoglycemia followed later by diabetes; thus, it is no longer used for prophylaxis.
Key Points
African trypanosomiasis is caused by Trypanosoma brucei gambiense in West and Central Africa and by T. b. rhodesiense in East Africa; tsetse flies are the main vector.
There are 3 stages of disease: cutaneous, hemolymphatic, and CNS (sleeping sickness).
Diagnose using light microscopy of blood (thin or thick smears) or another fluid sample.
Treatment of African trypanosomiasis varies by species and stage of disease.
T. b. gambiense and suramin for T. b. rhodesiense.
T. b. gambienseeflornithine is not available) for severe T. b. gambiense; and melarsoprol for T. b. rhodesiense.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.






