


Eight types of herpesviruses infect humans, two of which are herpes simplex viruses (HSV). Both types of herpes simplex virus, HSV-1 and HSV-2, can cause oral or genital infection. Most often, HSV-1 causes gingivostomatitis, herpes labialis, and herpes keratitis. HSV-2 usually causes genital lesions. (See Overview of Herpesvirus Infections.)
Transmission of HSV results from close contact with a person who is actively shedding virus. Viral shedding occurs from lesions but can occur even when lesions are not apparent.
After the initial infection, HSV remains dormant in nerve ganglia, from which it can periodically reactivate, causing symptoms. Recurrent herpetic eruptions are precipitated by
Overexposure to sunlight
Febrile illnesses
Physical or emotional stress
Immunosuppression
Unknown stimuli
Generally, recurrent eruptions are less severe and occur less frequently over time.
Diseases Caused by Herpes Simplex Virus
Diseases include
Mucocutaneous infection (most common), including genital herpes
Ocular infection (including herpes keratitis)
Central nervous system (CNS) infection
HSV rarely causes fulminant hepatitis in the absence of cutaneous lesions.
In patients with HIV infection, herpetic infections can be particularly severe. Progressive and persistent esophagitis, colitis, perianal ulcers, pneumonia, encephalitis, and meningitis may occur.
HSV outbreaks may be followed by erythema multiforme, possibly caused by an immune reaction to the virus.
Eczema herpeticum is a complication of HSV infection in which severe herpetic disease develops in skin regions with eczema.
Mucocutaneous herpes simplex infection
Lesions may appear anywhere on the skin or mucosa but are most frequent in the following locations:
Mouth or lips (perioral infection)
Genitals
Conjunctiva and cornea
Generally, after a prodromal period (typically < 6 hours in recurrent HSV-1) of tingling, discomfort, or itching, clusters of small, tense vesicles appear on an erythematous base. Clusters vary in size from 0.5 to 1.5 cm but may coalesce. Lesions on the nose, ears, eyes, fingers, or genitals may be particularly painful.
Vesicles typically persist for a few days, then rupture and dry, forming a thin, yellowish crust.
Healing generally occurs within 10 to 19 days after onset in primary infection or within 5 to 10 days in recurrent infection. Lesions usually heal completely, but recurrent lesions at the same site may cause atrophy and scarring. Skin lesions can develop secondary bacterial infection. In patients with depressed cell-mediated immunity due to HIV infection or other conditions, prolonged or progressive lesions may persist for weeks or longer. Localized infections can disseminate, particularly—and often dramatically—in patients who are immunocompromised.
Acute herpetic gingivostomatitis usually results from primary infection with HSV-1, typically in children. Herpetic pharyngitis can occur in adults as well as children. Through oral-genital contact, the cause can be either HSV-1 or HSV-2. Intraoral and gingival vesicles rupture, usually within several hours to 1 or 2 days, to form ulcers. Fever and pain often occur. Difficulty eating and drinking may lead to dehydration. After resolution, the virus resides dormant in the semilunar ganglion.
Herpes labialis is usually a recurrence of HSV. It develops as ulcers (cold sores) on the vermilion border of the lip or, much less commonly, as ulcerations of the mucosa of the hard palate.


Image courtesy of Dr. Herrmann via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Robert E. Sumpter via the Public Health Image Library of the Centers for Disease Control and Prevention.
Genital herpes is a common viral sexually transmitted infection and affected > 400 million people ages 15 to 49 years old worldwide in 2016 (see World Health Organization: Herpes Simplex Virus). Genital HSV can be caused by HSV-1 or HSV-2.
Herpes simplex keratitis
Herpes simplex keratitis (HSV infection of the corneal epithelium) causes pain, tearing, photophobia, and corneal ulcers that often have a branching pattern.
Herpetic whitlow

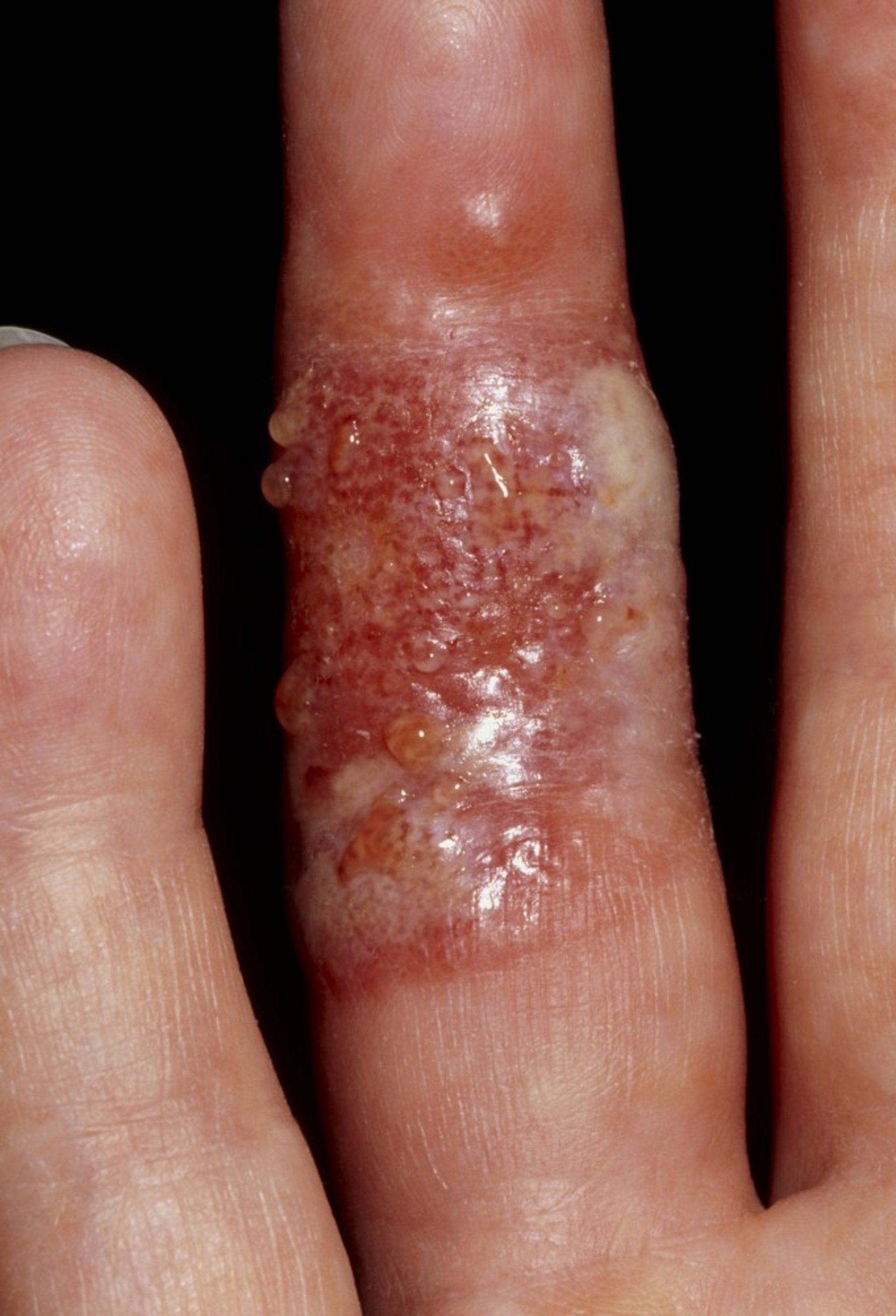
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Herpetic whitlow, a swollen, painful, erythematous lesion of the finger, results from inoculation of HSV through the skin and is most common among health care professionals.
Herpes simplex CNS infection
Herpes encephalitis occurs sporadically and may be severe. Multiple early seizures are characteristic.
Viral meningitis may result from HSV-2. It is usually self-limited.
Lumbosacral myeloradiculitis, typically caused by HSV-2, can occur during primary infection or reactivation of HSV-2 infection and can result in urinary retention or obstipation.
Neonatal herpes simplex
Neonatal HSV infection develops in neonates, including those whose mothers have no suggestion of current or past herpes infection. It is most commonly transmitted during birth through contact with vaginal secretions containing HSV and usually involves HSV-2.
Neonatal HSV infection usually develops between the 1st and 4th week of life, often causing mucocutaneous vesicles or central nervous system involvement. It causes major morbidity and mortality.
Diagnosis of Herpes Simplex Virus
History and physical examination
Sometimes laboratory confirmation
Polymerase chain reaction (PCR) of cerebrospinal fluid (CSF) and MRI for HSV encephalitis
Diagnosis of HSV infection is often clinical based on characteristic lesions.
Laboratory confirmation can be helpful, especially if infection is severe, the patient is immunocompromised or pregnant, or lesions are atypical. A Tzanck test (a superficial scraping from the base of a freshly ruptured vesicle stained with Wright-Giemsa stain) often reveals multinucleate giant cells in HSV or varicella-zoster virus infection.
Definitive diagnosis is with culture, seroconversion involving the appropriate serotype (in primary infections), PCR, and antigen detection. Fluid and material for culture should be obtained from the base of a vesicle or of a freshly ulcerated lesion. HSV can sometimes be identified using direct immunofluorescence assay of scrapings of lesions. PCR of CSF and MRI are used to diagnose HSV encephalitis.
HSV should be distinguished from herpes zoster, which rarely recurs and usually causes more severe pain and larger groups of lesions that are distributed along a dermatome and typically do not cross the midline.
Clusters of vesicles or ulcers on an erythematous base are unusual in genital ulcers other than those due to HSV infection.
If herpes infections recur frequently, do not resolve, or do not respond to antivirals as expected, immunocompromise, possibly due to HIV infection, should be suspected.
Treatment of Herpes Simplex Virus
Treating primary HSV infection with medications, even if done early, does not prevent the possibility of recurrence.
Mucocutaneous herpes simplex infection
Isolated infections often go untreated without consequence.
Gingivostomatitis and pharyngitis
Herpes labialis
Herpetic whitlow
Pearls & Pitfalls
|
Herpes simplex keratitis
Neonatal herpes simplex
Herpes simplex CNS infection
Key Points
HSV usually causes mucocutaneous infection but sometimes causes keratitis, and serious CNS infection can occur in neonates and in adults.
After initial infection, HSV remains dormant in nerve ganglia, from which it can periodically reactivate, causing symptoms.
Diagnose mucocutaneous infections clinically, but do viral culture, PCR, or antigen detection if patients are neonates, immunocompromised, or pregnant or have a CNS infection or severe disease.






