


Dysfunction of certain cranial nerves may affect the eye, pupil, optic nerve, or extraocular muscles and their nerves; thus, they can be considered cranial nerve disorders, neuro-ophthalmologic disorders, or both.
Neuro-ophthalmologic disorders may also involve dysfunction of the central pathways that control and integrate ocular movement and vision.
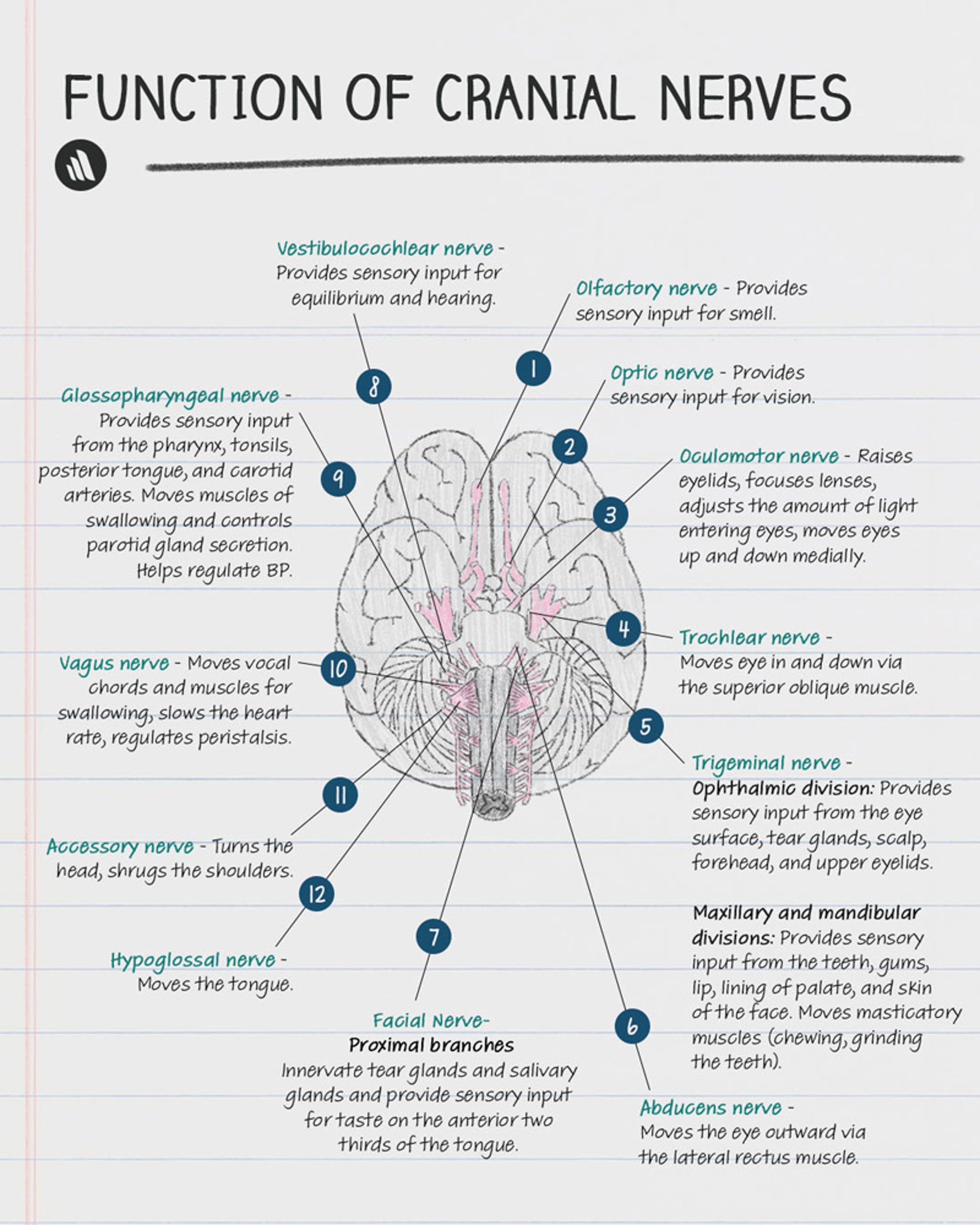
Cranial nerve disorders can also involve dysfunction of smell, vision, chewing, facial sensation or expression, taste, hearing, balance, swallowing, phonation, head turning and shoulder elevation, or tongue movements (see table Cranial Nerves). One or more cranial nerves may be affected.
(See also Horner Syndrome, Optic Nerve Disorders, and Approach to the Neurologic Patient.)

Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
Causes and symptoms of neuro-ophthalmologic and cranial nerve disorders overlap. Both types of disorders can result from tumors, inflammation, trauma, systemic disorders, and degenerative or other processes, causing such symptoms as vision loss, diplopia, ptosis, pupillary abnormalities, periocular pain, facial pain, or headache.
Diagnosis of Neuro-ophthalmologic and Cranial Nerve Disorders
Clinical evaluation
Neuroimaging
(See also How to Assess the Cranial Nerves.)
Evaluation of neuro-ophthalmologic and cranial nerve disorders includes the following:
Detailed questioning about symptoms
Tests to detect nystagmus
Visual system examination includes ophthalmoscopy and testing of visual acuity, visual fields, pupils, and eye movements (ocular motility). As part of this testing, the 2nd, 3rd, 4th, and 6th cranial nerves are examined. Neuroimaging with CT or MRI is also usually required.
The following parts of the visual examination are of particular interest in diagnosing neuro-ophthalmologic and cranial nerve disorders.
Pupils are inspected for size, equality, and regularity. Normally, the pupils constrict promptly (within 1 second) and equally during accommodation and during exposure to direct light and to light directed at the other pupil (consensual light reflex). Testing pupillary response to consensual light via a swinging flashlight test can determine whether a defect is present. Normally, the degree of pupillary constriction does not change as the flashlight is swung from eye to eye.
If a relative afferent defect (deafferented pupil, afferent pupillary defect, or Marcus Gunn pupil) is present, the pupil paradoxically dilates when the flashlight swings to the side of the defect. A deafferented pupil constricts in response to consensual but not to direct light.
If an efferent defect is present, the pupil responds sluggishly or does not respond to both direct and consensual light.
Eye movements are checked by having the patient hold the head steady while tracking the examiner’s finger as it moves to the far right, left, upward, downward, diagonally to either side, and inward toward the patient’s nose (to assess accommodation). However, such examination may miss mild paresis of ocular movement sufficient to cause diplopia.
Diplopia may indicate a defect in bilateral coordination of eye movements (eg, in neural pathways) or in the 3rd (oculomotor), 4th (trochlear), or 6th (abducens) cranial nerve. If diplopia persists when one eye is closed (monocular diplopia), the cause is probably a nonneurologic eye disorder. If diplopia disappears when either eye is closed (binocular diplopia), the cause is probably a disorder of ocular motility. The two images are furthest apart when the patient looks in the direction served by the paretic eye muscle (eg, to the left when the left lateral rectus muscle is paretic). The eye that, when closed, eliminates the more peripheral image is paretic. Placing a red glass over one eye can help identify the paretic eye. When the red glass covers the paretic eye, the more peripheral image is red.
Treatment of Neuro-ophthalmologic and Cranial Nerve Disorders
Treatment of the cause
Treatment of neuro-ophthalmologic and cranial disorders depends on the cause.






