


Meningiomas are tumors of the meninges that can compress adjacent brain tissue. Symptoms depend on the tumor’s location. Diagnosis is by MRI with contrast agent. Treatment may include excision, stereotactic radiosurgery, and sometimes radiation therapy.
Meningiomas, particularly those < 2 cm in diameter, are among the most common intracranial tumors. Meningiomas are the only brain tumor more common among women. These tumors tend to occur between ages 40 and 60 but can occur during childhood.
Meningiomas, which are usually benign, can develop wherever there is dura, most commonly over the convexities near the venous sinuses, along the base of the skull, and in the posterior fossa and rarely within ventricles. Multiple meningiomas may develop. Meningiomas compress but do not invade brain parenchyma. They can invade and distort adjacent bone.
There are many histologic types; all follow a similar clinical course, and some become malignant.
Symptoms and Signs of Meningiomas
Symptoms of meningiomas depend on which part of the brain is compressed and thus on the tumor’s location (see table Symptoms of Meningiomas by Site). Midline tumors in older people can cause dementia with few other focal neurologic findings.
Diagnosis of Meningiomas
MRI

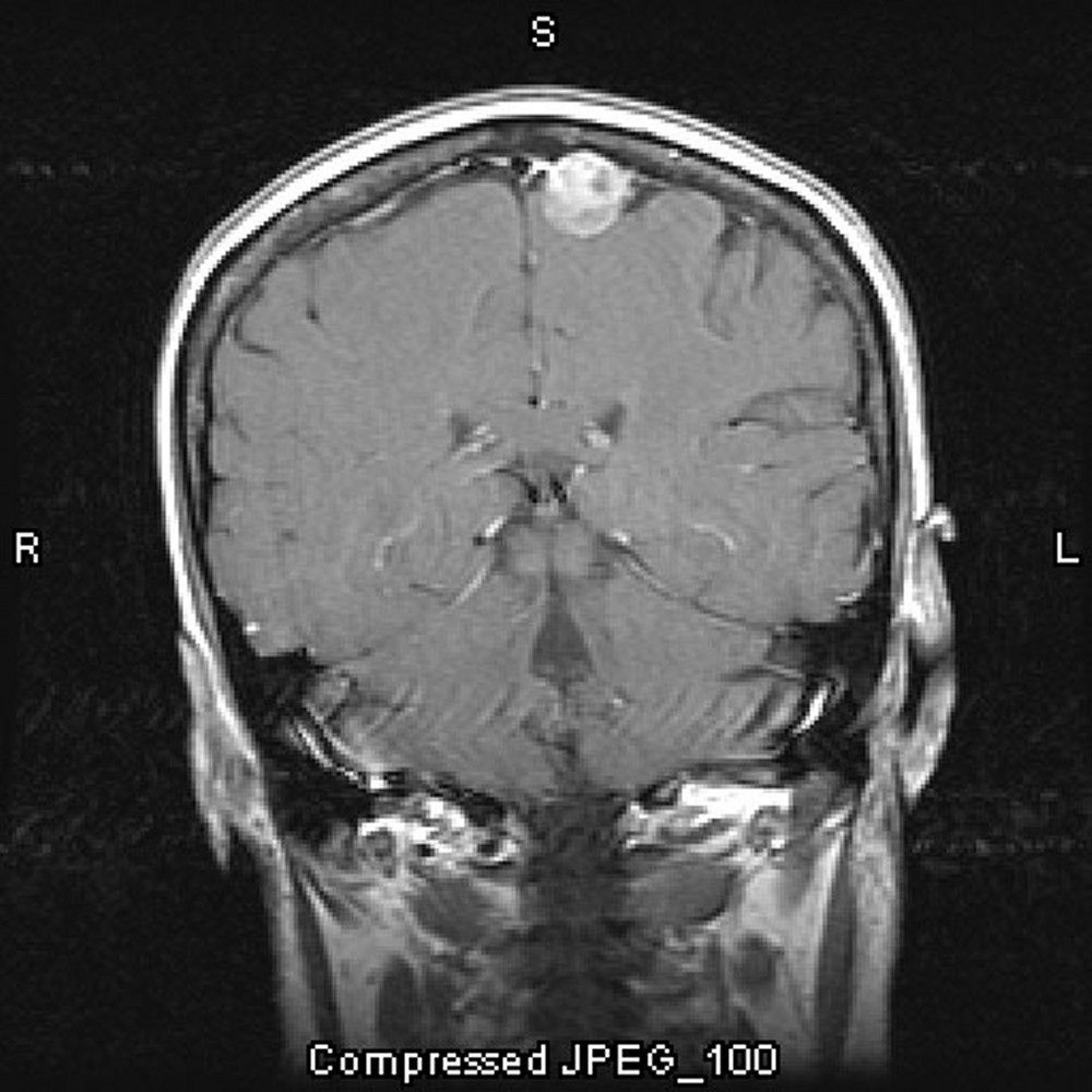
Image courtesy of William R. Shapiro, MD.
Diagnosis of meningiomas is similar to that of other brain tumors, usually by MRI with a paramagnetic contrast agent. Bone abnormalities (eg, brain atrophy, hyperostosis around the cerebral convexities, changes in the tuberculum sellae) may be seen incidentally on CT or plain x-rays.
Treatment of Meningiomas
For symptomatic or enlarging meningiomas, surgical excision or radiation therapy
For asymptomatic small meningiomas, particularly in older adults, monitoring with serial neuroimaging is sufficient.
Symptomatic or enlarging meningiomas should be excised if possible. In the following cases, surgery may cause more damage than the tumor and is thus deferred:
The meningiomas are large.
They encroach on blood vessels (usually surrounding veins).
They are close to critical brain areas (eg, brain stem).
Stereotactic radiosurgery is used for surgically inaccessible meningiomas and electively for other meningiomas. It is also used when tumor tissue remains after surgical excision or when patients are older.
If stereotactic radiosurgery is impossible or if a meningioma recurs, radiation therapy may be useful.
Key Points
Meningiomas are tumors of the meninges that are usually but not always benign.
They typically occur between ages 40 and 60 and are more common among women.
Symptoms vary greatly depending on the location of the tumor.
Excise symptomatic or enlarging tumors; use stereotactic radiosurgery if tumor remains after excision or cannot be excised completely.






