


Male sexual development and hormonal function depend on a complex feedback circuit involving the hypothalamus-pituitary-testes modulated by the central nervous system. Male sexual dysfunction can be secondary to hypogonadism, neurovascular or other disorders, or medication or recreational drug use.

Physiology
The hypothalamus produces gonadotropin-releasing hormone (GnRH), which is released in a pulsatile fashion every 60 to 120 minutes. Its target organ, the anterior pituitary gland, responds to each pulse of GnRH by producing a corresponding pulse of luteinizing hormone (LH) and, to a lesser degree, follicle-stimulating hormone (FSH). If the GnRH pulses do not occur with the proper amplitude, frequency, and diurnal variation, hypogonadism may result (idiopathic hypogonadotropic hypogonadism). Continuous (as opposed to pulsatile) stimulation by GnRH agonists (eg, as a treatment for advanced prostate cancer) actually suppresses pituitary release of LH and FSH and thus testosterone production.
The Leydig cells of the testes respond to LH by producing between 5 and 10 mg of testosterone daily. Testosterone levels are highest in early morning and lowest during the evening hours; however, in older men, this diurnal pattern may be blunted.
Testosterone is synthesized from cholesterol through several intermediate compounds, including dehydroepiandrosterone (DHEA) and androstenedione. Circulating testosteronetestosterone is bioavailable as free testosterone. This bioactive component of total testosterone is responsible for male characteristics, libido, bone and muscle mass.
In target tissues, about 4 to 8% of testosterone is converted to a more potent metabolite, dihydrotestosterone (DHT), by the enzyme 5-alpha-reductase. DHT has important trophic effects in the prostate and mediates androgenetic alopecia. In adults, spermatogenesis requires adequate intratesticular testosterone, but the role of DHT in spermatogenesis is unclear.
Testosterone and DHT have metabolic and other effects, including
Stimulating protein anabolism (increasing muscle mass and bone density)
Stimulating renal erythropoietin production (increasing red blood cell mass)
Stimulating bone marrow stem cells (modulating the immune system)
Causing cutaneous effects (ie, sebum production, hair growth)
Causing neural effects (ie, affecting cognition, increasing libido and possibly aggression)
Testosterone also undergoes conversion to estradiol by the enzyme aromatase; estradiol mediates most of testosterone's action on organs such as bones and the brain.
Testosterone, DHT, and estradiol provide negative feedback on the hypothalamic-pituitary axis. In males, estradiol is the main inhibitor of LH production, whereas both estradiol and inhibin B, a peptide produced by Sertoli cells of the testes, inhibit production of FSH. In the presence of testosterone, FSH stimulates the Sertoli cells and induces spermatogenesis. In spermatogenesis, each germinal cell (spermatogonium), located adjacent to the Sertoli cells, undergoes differentiation into 16 primary spermatocytes, each of which generates 4 spermatids. Each spermatid matures into a spermatozoon. Spermatogenesis takes 72 to 74 days and yields about 100 million new spermatozoa each day. Upon maturation, spermatozoa are released into the rete testis, where they migrate to the epididymis and eventually to the vas deferens. Migration requires an additional 14 days. During ejaculation, spermatozoa are mixed with secretions from the seminal vesicles, prostate, and bulbourethral glands.
Sexual Differentiation, Adrenarche, and Puberty
In the embryo, the presence of a Y chromosome triggers development and growth of the testes, which begin secreting testosterone and a müllerian duct inhibitor by about 7 weeks of gestation. Testosterone virilizes the wolffian duct (which develops into the epididymis, vas deferens, and seminal vesicles). Dihydrotestosterone promotes development of the male external genitals. Testosterone levels peak in the 2nd trimester and fall to almost zero by birth. Testosterone production rises briefly during the first 6 months of life, after which testosterone levels remain low until puberty. Müllerian inhibitory factor causes regression of the female genital organs in the fetus.
Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) are elevated at birth but fall to low levels within a few months, remaining low or undetectable throughout the prepubertal years. Through an unknown mechanism, blood levels of the adrenal androgens dehydroepiandrosterone (DHEA) and DHEA sulfate begin to increase several years before puberty. Their conversion to testosterone in small amounts initiates pubic and axillary hair growth (adrenarche). Adrenarche can occur as early as 9 or 10 years of age.
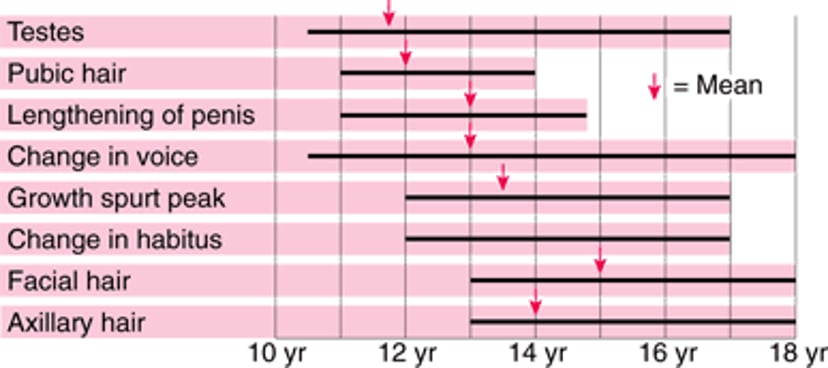
The mechanisms that initiate puberty are unclear, although early in puberty the hypothalamus becomes less sensitive to the inhibitory effects of sex hormones. This desensitization increases secretion of LH and FSH, corresponding to pulsatile gonadotropin-releasing hormone (GnRH) secretion, and stimulating testosterone and sperm production. In boys, the increased testosterone levels cause pubertal changes, the first of which is growth of the testes and scrotum. Later, penile length, muscle mass, and bone density increase; the voice deepens; and pubic and axillary hair becomes denser and thicker (see figure Puberty—when male sexual characteristics develop).
Puberty—when male sexual characteristics develop
Bars indicate normal ranges. No mean is available for change in habitus. |

Effects of Aging
Both hypothalamic secretion of gonadotropin-releasing hormone (GnRH) and the response of Leydig cells to follicle-stimulating hormone (FSH) and luteinizing hormone (LH) diminish with aging. In older people, Leydig cells decrease in number as well. Beginning at about age 30, a man’s serum total testosterone levels decline by 1 to 2% annually. Men aged 70 to 80 tend to have serum testosterone levels that are about one half to two thirds of those of men in their 20s. In addition, sex hormone–binding globulin (SHBG) levels increase with aging, causing an even greater decline in serum free and bioavailable testosterone. FSH and LH levels tend to be normal or high-normal. These age-related changes are referred to as the andropause, although there are no abrupt changes in hormone levels (and corresponding symptoms) as occur in menopause. The decline in testosterone may contribute to a combination of symptoms that has been termed androgen deficiency of the aging male (ADAM), which includes
Age-related muscle loss
Increased fat deposition
Osteopenia
Cognitive decline
If men have these symptoms plus low serum testosterone, they are diagnosed with hypogonadism
Testosterone supplementation in men with low-normal levels of testosterone is controversial. Some experts recommend a trial of testosterone supplementation in older men with symptoms or signs of hypogonadism and whose serum testosterone levels are slightly below the lower limit of normal. No data favor any of the testosterone preparations specifically for use in ADAM, although daily transcutaneous applications appear to be the most physiologic and best tolerated.






