


Hypogonadism is defined as testosterone deficiency with associated symptoms or signs, deficiency of spermatozoa production, or both. It may result from a disorder of the testes (primary hypogonadism) or of the hypothalamic-pituitary axis (secondary hypogonadism). Both may be congenital or acquired as the result of aging, disease, drugs, medications, or other factors. Additionally, a number of congenital enzyme deficiencies cause varying degrees of target organ androgen resistance. Diagnosis is confirmed by hormone levels. Treatment varies with etiology but typically includes gonadotropin-releasing hormone, gonadotropin, or testosterone replacement.
(See also Male Hypogonadism in Children.)
Etiology of Male Hypogonadism
Primary hypogonadism involves failure of the testes to respond to follicle-stimulating hormone (FSH) and luteinizing hormone (LH). When primary hypogonadism affects testosterone production, testosterone is insufficient to inhibit production of FSH and LH; hence, FSH and LH levels are elevated. The most common genetic cause of primary hypogonadism is Klinefelter syndrome. It involves seminiferous tubule dysgenesis, failure of spermatogenesis, Leydig cell hyperplasia, and a 47,XXY karyotype.
Secondary hypogonadism is failure of the hypothalamus to produce gonadotropin-releasing hormone (GnRH), as in idiopathic hypogonadotropic hypogonadism, or of the pituitary gland to produce enough FSH and LH. In secondary hypogonadism, testosterone levels are low and levels of FSH and LH are low or borderline normal. Any acute systemic illness can cause temporary secondary hypogonadism. Some syndromes of hypogonadism have both primary and secondary causes (mixed hypogonadism). The table Causes of Hypogonadism lists some common causes of hypogonadism by category.
Some syndromes of hypogonadism (eg, cryptorchidism, some systemic disorders) affect spermatozoon production more than testosterone levels.
Symptoms and Signs of Male Hypogonadism
Age at onset of testosterone deficiency (congenital, childhood-onset, or adult-onset hypogonadism) dictates the clinical presentation.
Congenital hypogonadism may be of 1st-, 2nd-, or 3rd-trimester onset. Congenital hypogonadism of 1st-trimester onset results in inadequate male sexual differentiation. Complete absence of testosterone’s effects results in normal-appearing female external genitals. Partial testosterone deficiency results in abnormalities ranging from ambiguous external genitals to hypospadias. Second- or 3rd-trimester onset of testosterone deficiency results in microphallus and undescended testes.
Childhood-onset testosterone deficiency (see Male Hypogonadism in Children) has few consequences and usually is unrecognized until puberty is delayed. Untreated hypogonadism impairs development of secondary sexual characteristics. As adults, affected patients have poor muscle development, a high-pitched voice, a small scrotum, decreased phallic and testicular growth, sparse pubic and axillary hair, and an absence of body hair. They may develop gynecomastia and eunuchoidal body proportions (arm span > height by 5 cm and pubic to floor length > crown to pubic length by > 5 cm) because of delayed fusion of the epiphyses and continued long bone growth.
Adult-onset testosterone deficiency has varied manifestations depending on the degree and duration of the deficiency. Decreased libido; erectile dysfunction; decline in cognitive skills, such as visual-spatial interpretation; sleep disturbances; vasomotor instability (in acute, severe male hypogonadism); and mood changes, such as depression and anger, are common. Decreased lean body mass, increased visceral fat, testicular atrophy, osteopenia, gynecomastia, and sparse body hair typically take months to years to develop. Testosterone deficiency may increase the risk of coronary artery disease and prostate cancer.
Diagnosis of Male Hypogonadism
Testing, beginning with follicle-stimulating hormone (FSH), luteinizing hormone (LH), and testosterone levels
Congenital and childhood-onset hypogonadism are often suspected because of developmental abnormalities or delayed puberty. Adult-onset hypogonadism should be suspected on the basis of symptoms or signs but is easily missed because these clinical markers are insensitive and nonspecific. Klinefelter syndrome should be considered in adolescent males in whom puberty is delayed, young men with hypogonadism, and all adult men with very small testes. Hypogonadism requires confirmatory testing (see figure Laboratory Evaluation of Male Hypogonadism).
Diagnosis of primary and secondary hypogonadism
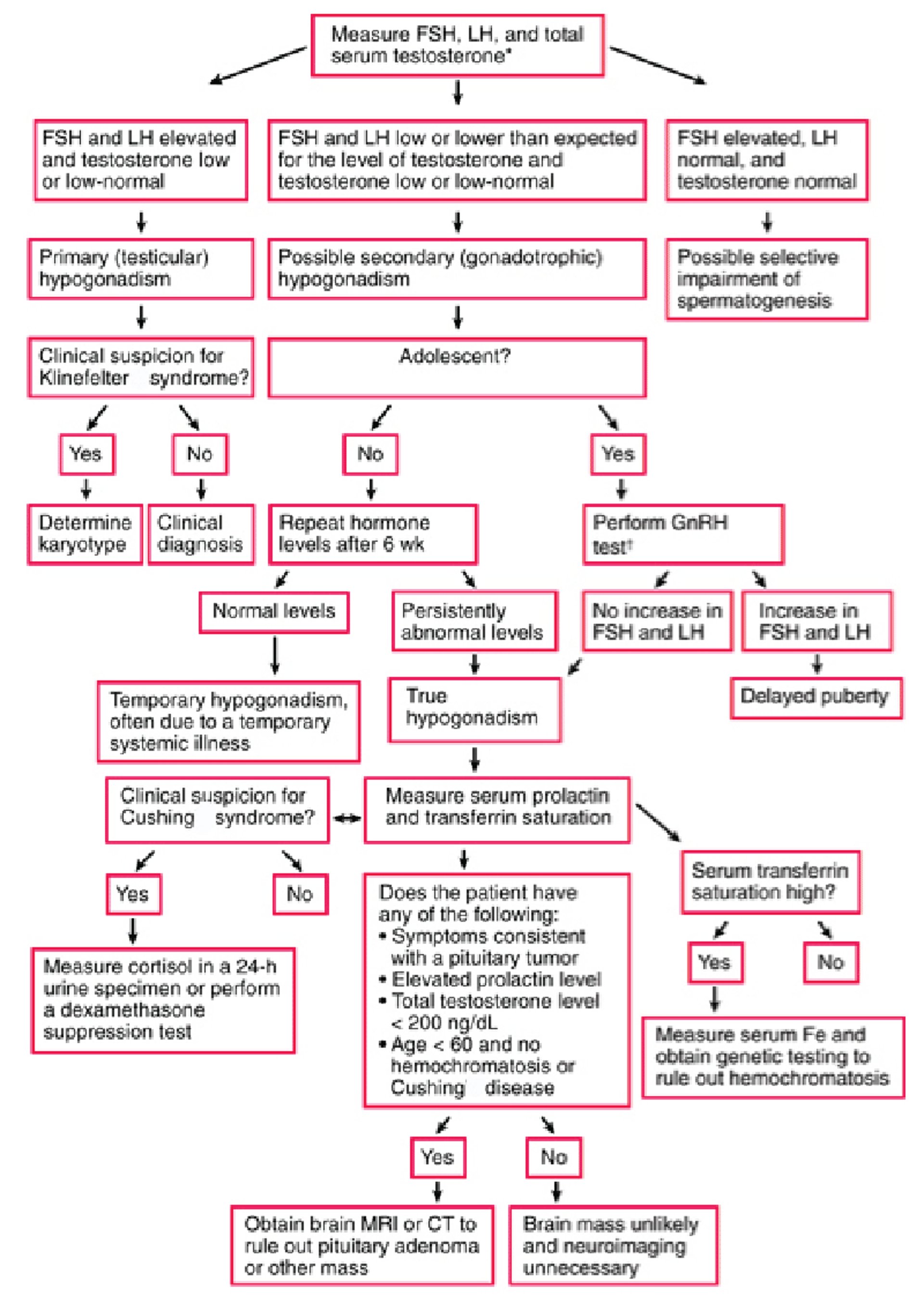
Increases in FSH and LH are more sensitive for primary hypogonadism than are decreases in testosterone levels. Levels of FSH and LH also help determine whether hypogonadism is primary or secondary. High gonadotropin levels, even with low-normal testosterone levels, indicate primary hypogonadism, whereas gonadotropin levels that are low or lower than expected for the level of testosterone indicate secondary hypogonadism. Alternatively, in boys of short stature with delayed puberty, low testosterone plus low gonadotropin levels might result from constitutional delay of puberty. Elevation of serum FSH with normal levels of serum testosterone and LH often occurs when spermatogenesis is impaired but testosterone production is normal. The cause of hypogonadism is often evident clinically. Primary hypogonadism requires no further testing, although some clinicians do a karyotype to definitively diagnose Klinefelter syndrome.
Total (and, when possible, free) serum testosterone, serum FSH, and serum LH levels are measured simultaneously. The normal range for total testosterone is 300 to 1000 ng/dL (10.5 to 35 nmol/L). The testosterone level should be drawn in the morning (before 10:00 AM) to confirm hypogonadism. Because of the increase in sex hormone–binding globulin (SHBG) with aging, total testosterone level is a less sensitive indicator of hypogonadism after age 50. Although serum free testosterone more accurately reflects functional testosterone levels, its measurement requires equilibrium dialysis, which is technically difficult and not widely available.
Some commercially available kits, including the analog free testosterone assay, attempt to measure serum free testosterone levels, but the results are often inaccurate, particularly in conditions (such as type 2 diabetes, obesity, and hypothyroidism) that alter SHBG levels. Free testosteronetestosterone values; there are calculators available online. See the Free and Bioavailable Testosterone Calculator.
Because of the pulsatile secretion of FSH and LH, these hormones are have been measured as a pooled sample of 3 venipunctures taken at 20-minute intervals, but these pooled samples seldom add clinically important information compared with a single blood sample. Serum FSH and LH levels are usually ≤ 5 mIU/mL (5 IU/L) before puberty and between 5 and 15 mIU/mL (5 and 15 IU/L) in adulthood.
Semen analysis should be done in all men who are seeking fertility treatment. In adolescents or adults, a semen sample collected by masturbation after 2 days of abstinence from ejaculation provides an excellent index of seminiferous tubular function. A normal semen sample (World Health Organization [WHO] standards) has a volume of > 1.5 mL with > 15 million sperm/mL, of which 50% are of normal morphology and are motile (see also Sperm Disorders).
Laboratory evaluation of male hypogonadism
† Recommended by some physicians. CT = computed tomography; Fe = iron; FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; LH = luteinizing hormone; MRI = magnetic resonance imaging. |

Evaluation of secondary hypogonadism
Because any systemic illness can temporarily decrease levels of testosterone, FSH, and LH, secondary hypogonadism should be confirmed by measuring these levels again at least 4 weeks after resolution of the systemic illness. To confirm secondary hypogonadism in adolescents, the GnRH stimulation test may be considered. If levels of FSH and LH increase in response to IV GnRH, puberty is simply delayed. If levels do not increase, true hypogonadism is likely.
To help determine the cause of confirmed secondary hypogonadism, testing should include serum prolactin level (to screen for pituitary adenoma) and transferrin saturation (to screen for hemochromatosis). Sella imaging with MRI or CT is done to exclude a pituitary macroadenoma or other mass in men with any of the following:
Age < 60 years with no other identified cause for hypogonadism
Very low total testosterone levels (< 200 ng/dL [6.94 nmol/L])
Elevated prolactin levels
Symptoms consistent with a pituitary tumor (eg, headache, visual symptoms)
Also, if there are symptoms or signs of Cushing syndrome, 24-hour urine collection for free cortisol or a dexamethasone suppression test is done. If no abnormalities are identified, the diagnosis is acquired idiopathic secondary hypogonadism.
Treatment of Male Hypogonadism
Gonadotropin replacement therapy for restoration of fertility due to secondary hypogonadism
Treatment is directed toward providing adequate androgen replacement conveniently and safely. Although patients with primary hypogonadism may not become fertile with any endocrine therapy, patients with secondary hypogonadism often become fertile with gonadotropin therapy. Testosterone formulations discussed here are those available in the US. Other formulations may be available in other countries.
Testosterone replacement therapy (TRT)
Because exogenous testosterone impairs spermatogenesis, TRT should be avoided, when possible, when subsequent fertility is a concern (unless there is irreversible primary testicular failure), including in secondary hypogonadism. However, if subsequent fertility is not a concern, testosterone replacement therapy alone may be used to treat secondary hypogonadism. Treatment of secondary hypogonadism in boys with gonadotropin replacement therapy (see Treatment of infertility due to hypogonadism) usually stimulates androgen production as well as spermatogenesis.
TRT can be used for young males who
Have no signs of puberty
Are near age 15
Have had secondary hypogonadism excluded
testosterone
Adults with established testosterone deficiency may benefit from replacement therapy. Treatment slows the course of osteopenia, muscle loss, vasomotor instability, loss of libido, depression, and occasionally erectile dysfunction. The effects of testosterone on coronary artery disease
testosterone daily)
Transdermal axillary solution (60 mg once a day)
A buccal mucosal lozenge (30 mg twice a day)
A nasal formulation (one spray of 5.5 mg in each nostril 3 times a day)
Testosterone gel maintains physiologic blood levels more consistently than other treatments, but IM or patch systems are sometimes preferred because of their lower cost. Oral formulations are unpredictably absorbed.
Potential adverse effects of testosterone and its analogs include
Erythrocytosis (particularly in men over age 50 receiving IM testosterone)
Venous thromboembolism unrelated to erythrocytosis
testosterone to physiologic levels is not thought to cause new prostate cancer or accelerate growth or spread of localized prostate cancer. TRT is thought to have a minimal effect on serum prostate-specific antigen (PSA) levels in men with benign prostatic hyperplasia and in men with treated prostate cancer. However, product inserts do state that TRT is contraindicated in men with prostate cancer, and men who have or are at high risk of prostate cancer should be counseled and carefully followed with digital rectal examinations and PSA measurements while taking TRT. A prostate biopsy may be needed if PSA elevation persists after TRT is stopped. Hypogonadal men with effectively treated prostate cancer or suspected of having prostate cancer should seek consultation with an expert.
Men taking supplemental testosterone should be monitored periodically. Hematocrit (Hct), PSA, and testosterone levels should be measured quarterly during the first year of TRT and semiannually thereafter. Digital rectal examination should be offered at the same times. If Hct is ≥ 54%, the testosterone dose should be reduced. Significant increases in PSA level should prompt consideration of prostate biopsy in men who would otherwise be candidates for prostate cancer diagnosis and treatment.
Treatment of infertility due to hypogonadism
Infertility has many possible causes other than hypogonadism. Infertility due to primary hypogonadism (elevated FSH) does not respond to hormonal therapy. Men with primary hypogonadism occasionally have a few intratesticular sperm that can be harvested with various microsurgical techniques and used to fertilize an egg by assisted reproductive technique (eg, intracytoplasmic sperm injection).
Infertility due to secondary hypogonadism usually responds to gonadotropin replacement therapy. Other symptoms of secondary hypogonadism also respond well to testosteronetestosterone. Once an adequate sperm count is achieved, FSH can be stopped and hCG monotherapy continued.
Most men who have secondary hypogonadism due to a hypothalamic defect (eg, idiopathic hypogonadotropic hypogonadism, Kallmann syndrome) become fertile with treatment despite sperm counts that are low (eg, < 5 million/mL). When LH and FSH treatment is ineffective, pulsatile gonadotropin-releasing hormone replacement therapy (every 2 hours subcutaneous by a programmable minipump), although less readily available, might be more effective. Most (80 to 90%) of men respond successfully to these regimens.
Key Points
Levels of FSH and LH help differentiate between primary hypogonadism (high levels) and secondary hypogonadism (low or borderline normal levels).
Age-related symptoms of male hypogonadism include inadequate sexual differentiation (congenital), delayed puberty (childhood onset), and various nonspecific symptoms such as decreased libido, erectile dysfunction, cognitive decline, decrease in percentage of lean body mass, sleep disturbances, and mood changes (adult onset).
Free testosterone levels, which can be calculated and sometimes measured, better reflect gonadal sufficiency than do total testosterone levels.
Diagnosis can be approached systematically, using an algorithm.
Gonadotropin replacement therapy can usually restore fertility in men with secondary hypogonadism.






