


Abnormal vaginal or uterine bleeding includes
Menses that are excessive in frequency (amenorrhea, oligomenorrhea, polymenorrhea), volume, or duration (menorrhagia, or heavy menstrual bleeding)
Bleeding that occurs between menses (intermenstrual bleeding) or is unrelated to menses and occurs irregularly (metrorrhagia)
Premenarchal bleeding
Postmenopausal bleeding (ie, > 12 months after the last normal menses)
Vaginal bleeding may also occur during early pregnancy or during late pregnancy.
Vaginal bleeding can originate anywhere in the genital tract, including the vulva, vagina, cervix, and uterus. When vaginal bleeding originates in the uterus, it is called abnormal uterine bleeding (AUB).
Pathophysiology of Vaginal Bleeding
Most abnormal vaginal bleeding involves
Hormonal abnormalities in the hypothalamic-pituitary-ovarian axis
Structural (eg, uterine fibroids) or inflammatory (eg, chronic endometritis) disorders
Gynecologic cancers
Bleeding disorders (uncommon)
With hormonal causes, ovulation does not occur or occurs infrequently or irregularly. During an anovulatory cycle, the corpus luteum does not form, and thus the normal cyclical secretion of progesterone does not occur. Without progesterone, estrogen causes the endometrium to continue to proliferate, eventually outgrowing its blood supply. The endometrium then sloughs and bleeds incompletely, irregularly, and sometimes profusely or for a long time. Structural disorders (eg, uterine fibroids) may cause abnormal bleeding because they interfere with the function of the uterine muscle (myometrium).
Etiology of Vaginal Bleeding
Causes of vaginal bleeding in adults (see table Some Causes of Vaginal Bleeding in Adult Women) and children (see table Common Causes of Vaginal Bleeding in Children) vary.
During the reproductive years, common causes of vaginal bleeding include
Complications of an early, undiagnosed pregnancy
Submucous myoma
Endometrial or cervical polyps
Midcycle bleeding associated with ovulation
Breakthrough bleeding while women are taking oral contraceptives
Ovulatory dysfunction is the most common cause of abnormal uterine bleeding (AUB) during the reproductive years.
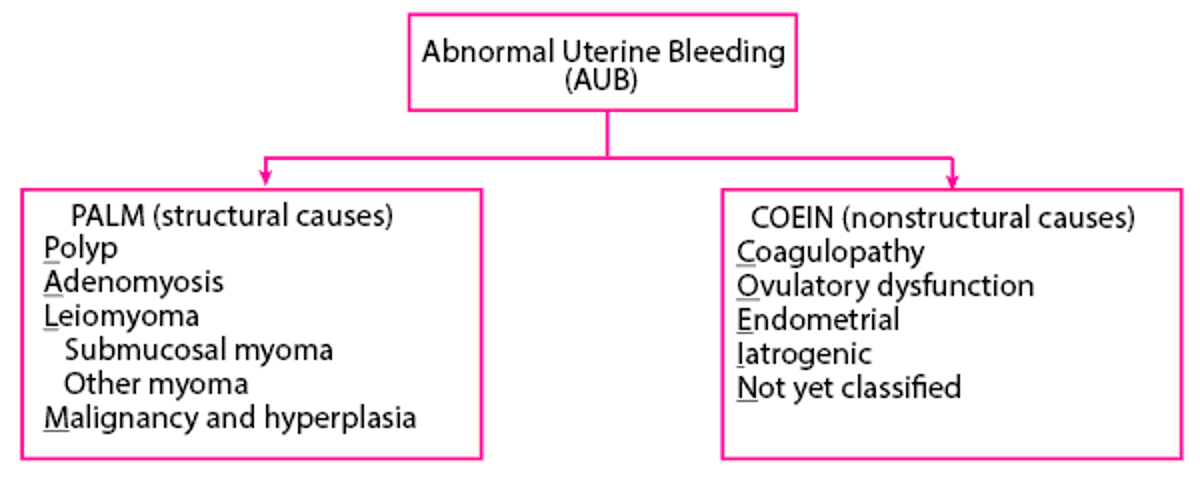
Causes of AUB in nonpregnant women of reproductive age may be classified as structural or nonstructural as in the PALM-COEIN classification system (1, 2). PALM-COEIN is a mnemonic for the structural causes (PALM) and the nonstructural (COEIN) causes.
Vaginitis, foreign bodies, and trauma are common causes of vaginal bleeding before menarche. Sexual abuse and cancer are less common causes; however, prompt evaluation is required to rule these condition out.
PALM-COEIN Classification System

Etiology references
1. Practice bulletin no. 128: Diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol 120 (1):197-206, 2012. doi: 10.1097/AOG.0b013e318262e320
2. Practice bulletin no. 136: Management of abnormal uterine bleeding associated with ovulatory dysfunction. Obstet Gynecol 122 (1):176-185, 2013. doi: 10.1097/01.AOG.0000431815.52679.bb
Evaluation of Vaginal Bleeding
The first priority is determining whether the patient has persistent major bleeding or is at risk of it (eg, due to ectopic pregnancy).
Unrecognized pregnancy must be suspected and diagnosed in women of reproductive age because some causes of vaginal bleeding during pregnancy (eg, ectopic pregnancy) are life threatening.
History
History of present illness should include quantity (eg, by number of pads used per day or hour) and duration of bleeding, as well as the relationship of bleeding to menses and sexual activity. Clinicians should ask about the following:
Menstrual history, including date of last normal menstrual period, age at menarche and menopause (when appropriate), cycle length and regularity, quantity and duration of typical menstrual bleeding, and the frequency of dysmenorrhea
Previous episodes of abnormal bleeding, including frequency, duration, quantity, and pattern (cyclicity) of bleeding
Sexual history, including possible history of sexual assault
Review of systems should seek symptoms of possible causes, including the following:
Missed menses, breast swelling, and nausea: Pregnancy-related bleeding
Abdominal pain, sometimes with light-headedness or syncope: Ectopic pregnancy or ruptured ovarian cyst
Chronic pelvic or abdominal pain, bloating, change in bowel habits, or weight loss: Gynecologic cancer
Easy bruising and excessive bleeding during toothbrushing, minor lacerations, or venipuncture: A bleeding disorder
Past medical history should identify disorders known to cause vaginal bleeding, including a recent spontaneous or induced abortion or structural disorders (eg, uterine fibroids, cervical or endometrial polyps). Clinicians should identify risk factors for: endometrial cancer (including obesity, diabetes, prolonged estrogen use without a progestin), cervical cancer (including abnormal or inadequate cervical cancer screening, immunosuppression), and polycystic ovary syndrome.
Drug history should include specific questions about use of hormonal contraceptives, other hormones, and other drugs that may cause AUB (eg, anticoagulants, nonsteroidal anti-inflammatory drugs).
Family history of bleeding problems or gynecologic cancers should be queried.
If sexual abuse of a child is suspected, a structured forensic interview based on the National Institute of Child Health and Human Development (NICHD) Protocol can be used. It helps the child report information about the experienced event and improves the quality of information obtained.
Physical examination
Vital signs are reviewed for signs of hypovolemia (eg, tachycardia, hypotension).
During the general examination, clinicians should look for signs of anemia (eg, conjunctival pallor) and evidence of possible causes of abnormal uterine bleeding, including the following:
Hirsutism, acne, obesity, and enlarged ovaries: Polycystic ovary syndrome
Warm and moist or dry skin, eye abnormalities, tremor, abnormal reflexes, or goiter: A thyroid disorder
Nipple discharge: Hyperprolactinemia
Low body mass index: Possibly hypothalamic anovulation
Hepatomegaly, jaundice, asterixis (flapping tremor of the wrist), or splenomegaly: A liver disorder
Easy bruising, petechiae, purpura, or mucosal (eg, gingival) bleeding: A bleeding disorder
Abdominal mass or ascites: Cancer, including gynecologic cancers
In children, breast development and presence of pubic and axillary hair at a younger age than is typical for puberty: Precocious puberty
In children, difficulty walking or sitting; bruises or tears around the genitals, anus, or mouth; and/or vaginal discharge or pruritus: Sexual abuse
The abdomen is examined for distention, tenderness, and masses (particularly an enlarged uterus).
A pelvic examination is done. External inspection and speculum examination help identify lesions of the vulva, vagina, cervix, and urethra. Bimanual examination is done to evaluate uterine size and ovarian enlargement. If abdominal examination suggests a late-stage pregnancy, digital cervical examination is contraindicated until placental position is determined. If no blood is present in the vagina, rectal examination is done to determine whether bleeding is gastrointestinal in origin.
If a child cannot tolerate a pelvic examination or if the source if the child's bleeding is undetermined, the child may be given an anesthetic before the examination; vaginoscopy is done if necessary to examine the vagina and cervix.
Red flags
The following findings are of particular concern:
Excessive bleeding
Hemodynamic instability (tachycardia, hypotension)
Premenarchal or postmenopausal vaginal bleeding
Vaginal bleeding in pregnant patients
In children, difficulty walking or sitting; bruises or tears around the genitals, anus, or mouth; and/or vaginal discharge or pruritus suggestive of sexual abuse.
Interpretation of findings
Significant hypovolemia or hemorrhagic shock is unlikely except with ruptured ectopic pregnancy or, rarely, a ruptured ovarian cyst.
In children, breast development and pubic or axillary hair before the typical age range for puberty suggest precocious puberty and premature menses. In those without such findings, the possibility of sexual abuse should be investigated unless an explanatory lesion or foreign body is obvious.
In women of reproductive age, examination may detect a causative gynecologic lesion or other findings suggesting a cause. If younger patients taking hormonal contraceptives have no apparent abnormalities during examination and bleeding is spotty, bleeding may be related to the hormones. If the problem is excessive menstrual bleeding only, a uterine disorder or bleeding diathesis should be considered. Inherited bleeding disorders may initially manifest as heavy menstrual bleeding beginning at menarche or during adolescence.
In postmenopausal women, gynecologic cancer should be suspected.
Testing
All patients of reproductive age require
A urine or blood pregnancy test
Vaginal bleeding during pregnancy requires a specific approach (see Vaginal Bleeding During Early Pregnancy and Vaginal Bleeding During Late Pregnancy).
Blood tests include a complete blood count (CBC) if bleeding is unusually heavy (eg, > 1 pad or tampon/hour) or has lasted > 7 days or if findings suggest anemia or hypovolemia. If anemia is identified and is not obviously due to iron deficiency (eg, based on microcytic, hypochromic red blood cell [RBC] indices), iron studies are done.
Thyroid-stimulating hormone and prolactin levels are usually measured, even when galactorrhea is absent.
If polycystic ovary syndrome is suspected, testosterone and dehydroepiandrosterone sulfate (DHEAS) levels are measured.
Imaging includes transvaginal ultrasonography if women have any of the following:
A suspected structural lesion (based on history or examination)
Focal thickening of the endometrium that is detected during screening ultrasonography may require hysteroscopy or saline-infusion sonohysterography to identify small uterine masses (eg, endometrial polyps, submucous myomas).
Other testing includes endometrial sampling if examination and ultrasonography are inconclusive in patients with any of the following:
Age > 45
Unopposed estrogen exposure (as occurs in women with a high body mass index or polycystic ovary syndrome)
Risk factors for gynecologic cancer
Endometrial thickening > 4 mm in postmenopausal patients
Sampling can be done by endometrial biopsy or, if the cervical canal requires dilation, by dilation and curettage (D & C).
Treatment of Vaginal Bleeding
Hemorrhagic shock requires immediate treatment, often via laparoscopy or laparotomy. Women with iron deficiency anemia may require supplemental oral iron.
Definitive treatment of vaginal bleeding is directed at the cause. Typically, hormones, usually oral contraceptives, are first-line treatment for abnormal uterine bleeding due to ovulatory dysfunction.
Geriatrics Essentials
Postmenopausal bleeding (bleeding > 12 months after the final menstrual period) is abnormal and requires further evaluation to exclude cancer, unless it clearly results from withdrawal of exogenous hormones.
In women not taking exogenous hormones, the most common cause of postmenopausal bleeding is endometrial atrophy, but endometrial pathology should still be ruled out.
In some older women, physical examination of the vagina can be difficult because lack of estrogen leads to increased friability of the vaginal mucosa, vaginal stenosis, and sometimes adhesions in the vagina. For these patients, a pediatric speculum may be more comfortable.
Key Points
Pregnancy must be excluded in women of reproductive age even when history does not suggest it.
Ovulatory dysfunction is the most common cause of abnormal uterine bleeding during the reproductive years.
Vaginitis, foreign bodies, and trauma are common causes of vaginal bleeding before menarche; sexual abuse is a less common cause but, if suspected, requires prompt evaluation.
Postmenopausal vaginal bleeding needs further evaluation to exclude cancer.






