Voiding disorders affect urine storage or release because both are controlled by the same neural and urinary tract mechanisms. The result is incontinence or retention.
For normal urinary function, the autonomic and voluntary nervous systems must be intact, and muscles of the urinary tract must be functional. Normally, bladder filling stimulates stretch receptors in the bladder wall to send impulses via spinal nerves S2 to S4 to the spinal cord, then to the sensory cortex, where the need to void is perceived. A threshold volume, which differs from person to person, triggers awareness of the need to void. However, the external urinary sphincter at the bladder outlet is under voluntary control and usually remains contracted until a person decides to urinate.
The micturition inhibitory center in the frontal lobe also helps control urination. When the decision is made, voluntary signals in the motor cortex initiate urination. These impulses are transmitted to the pontine micturition center, which coordinates simultaneous signals to contract detrusor smooth muscle throughout the bladder (via parasympathetic cholinergic nerve fibers) and to relax the internal sphincter (via alpha sympathetic nerve fibers) and striated muscle of the external sphincter and pelvic floor (see figure Normal Micturition: Coordinated Bladder Contraction and Urethral Sphincter Relaxation). In addition to normal urinary function, continence and normal voiding require normal cognitive function (including motivation), mobility, access to a toilet, and manual dexterity.
Damage to or dysfunction of any of the components involved in voiding can cause urinary incontinence or retention.
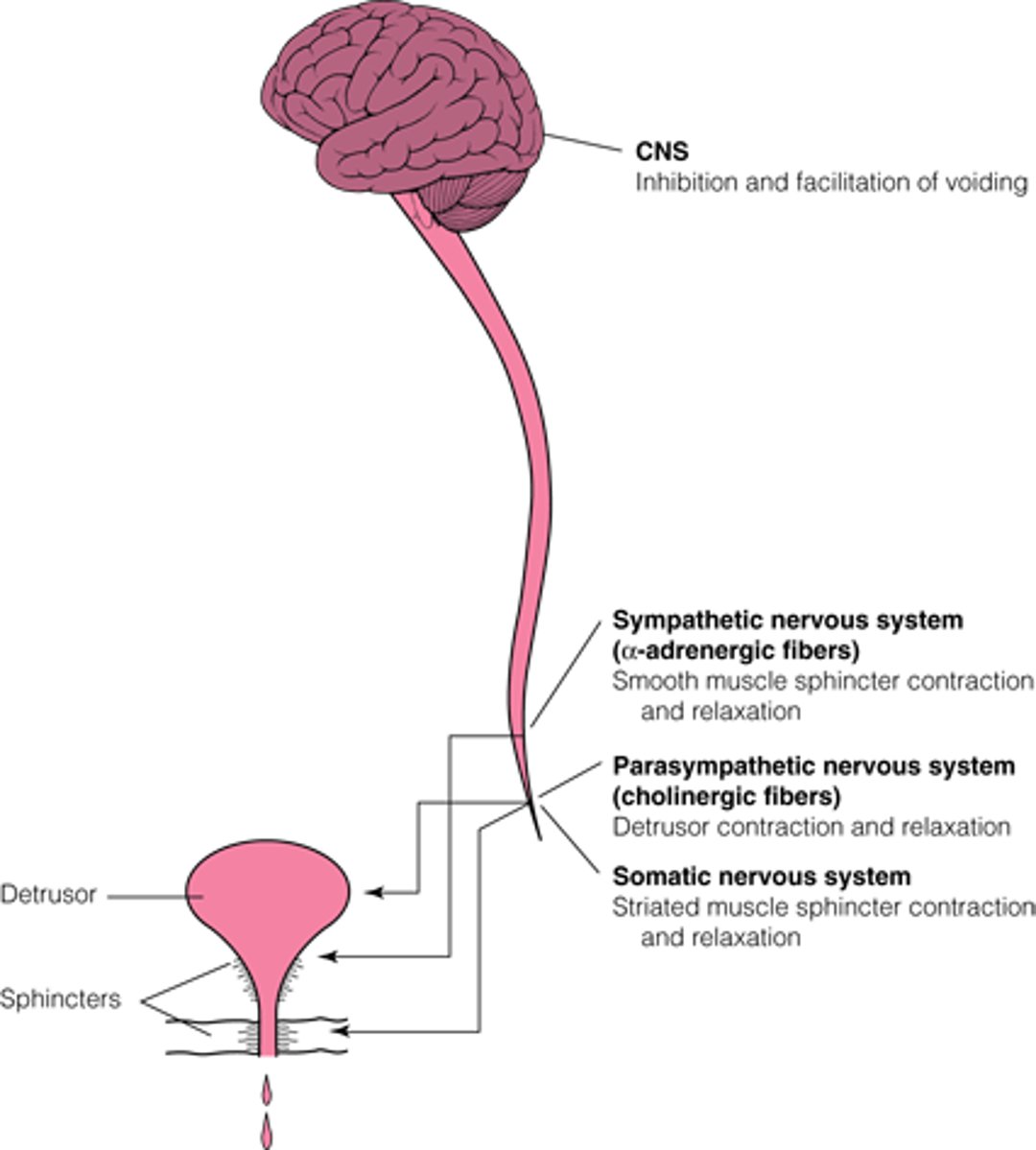
Normal Micturition: Coordinated Bladder Contraction and Urethral Sphincter Relaxation
The CNS inhibits voiding until the appropriate time and coordinates and facilitates input from the lower urinary tract to start and complete voiding. The sympathetic system contracts the smooth muscle sphincter. The parasympathetic nervous system contracts the bladder detrusor muscle through cholinergic fibers. The somatic nervous system contracts the striated muscle sphincter through cholinergic fibers from the pudendal nerve. (Adapted from DuBeau CE, Resnick NM with the Massachusetts Department of Health EDUCATE project collaborators: Urinary Incontinence in the Older Adult: An Annotated Speaker/Teacher Kit, 1993; used with permission of the authors.) |