


Renal atheroembolism is occlusion of renal arterioles by atherosclerotic emboli, causing progressive chronic kidney disease. It results from rupture of atheromatous plaques. Symptoms are those of renal failure; symptoms and signs of widespread arterial embolic disease may be present. Diagnosis is by renal biopsy. Long-term prognosis is usually poor. Treatment aims to prevent further embolization.
Atheromatous plaque rupture usually results from manipulation of the aorta or other large arteries during vascular surgery, angioplasty, or arteriography. Spontaneous plaque rupture, which occurs most often in patients who have diffuse erosive atherosclerosis or who are being treated with anticoagulants or fibrinolytics, is rare.
Atheroemboli tend to cause incomplete occlusion with secondary ischemic atrophy rather than renal infarction. A foreign body immune reaction often follows embolization, leading to continued deterioration in renal function for 3 to 8 weeks. Acute renal impairment may also result from massive or recurrent episodes of embolization.
Symptoms and Signs of Renal Atheroembolism
Symptoms are usually those of acute or chronic renal dysfunction with uremia (see Acute Kidney Injury [AKI]: Symptoms). Abdominal pain, nausea, and vomiting can result from concomitant compromised arterial microcirculation of abdominal organs (eg, pancreas, gastrointestinal tract). Sudden blindness and formation of bright yellow retinal plaques (Hollenhorst plaques) can result from emboli in retinal arterioles.
Signs of widespread peripheral embolism (eg, livedo reticularis, painful muscle nodules, overt gangrene, which is often referred to as the trash syndrome) are sometimes present.
Diagnosis of Renal Atheroembolism
Clinical suspicion
Sometimes, renal biopsy
Location of source of emboli
Diagnosis is suggested by worsening renal function in a patient with recent manipulation of the aorta, particularly if there are signs of atheroemboli. Differential diagnosis includes contrast-induced and drug-induced nephropathy.
If suspicion of atheroembolism remains high, percutaneous renal biopsy is done; it has a sensitivity of about 75%. Diagnosis is important because there may be treatable causes of emboli in the absence of vascular obstruction. Cholesterol crystals in the emboli dissolve during tissue fixation, leaving pathognomonic biconcave, needle-shaped clefts in the occluded vessel. Sometimes skin, muscle, or gastrointestinal biopsy can provide the same information and indirectly help establish the diagnosis.

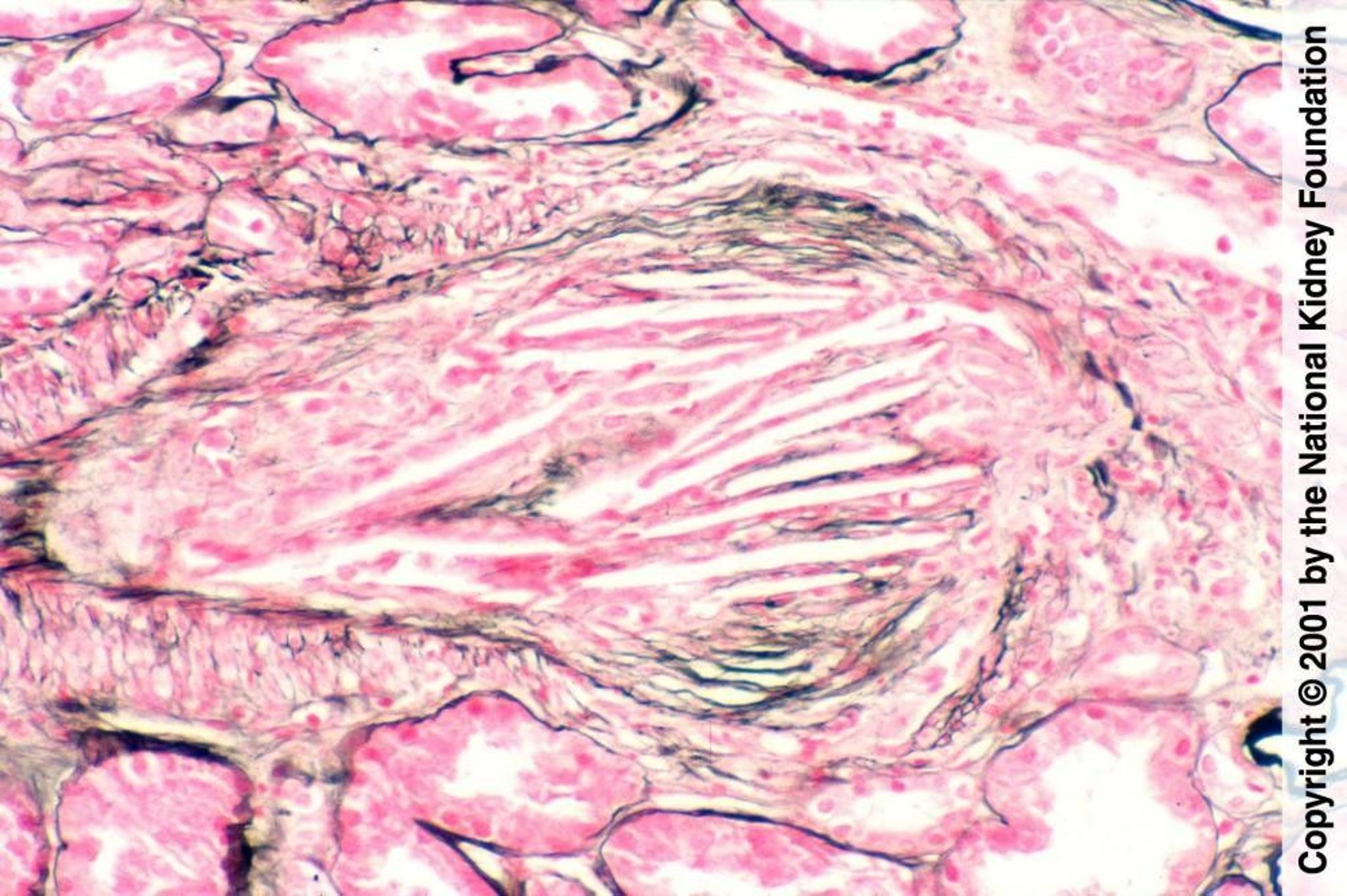
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Blood and urine tests can confirm the diagnosis of acute kidney injury or chronic kidney disease but do not establish cause. Urinalysis typically shows microscopic hematuria and minimal proteinuria; however, proteinuria is occasionally in the nephrotic range (> 3 g/day). Eosinophilia, eosinophiluria, and transient hypocomplementemia may be present.

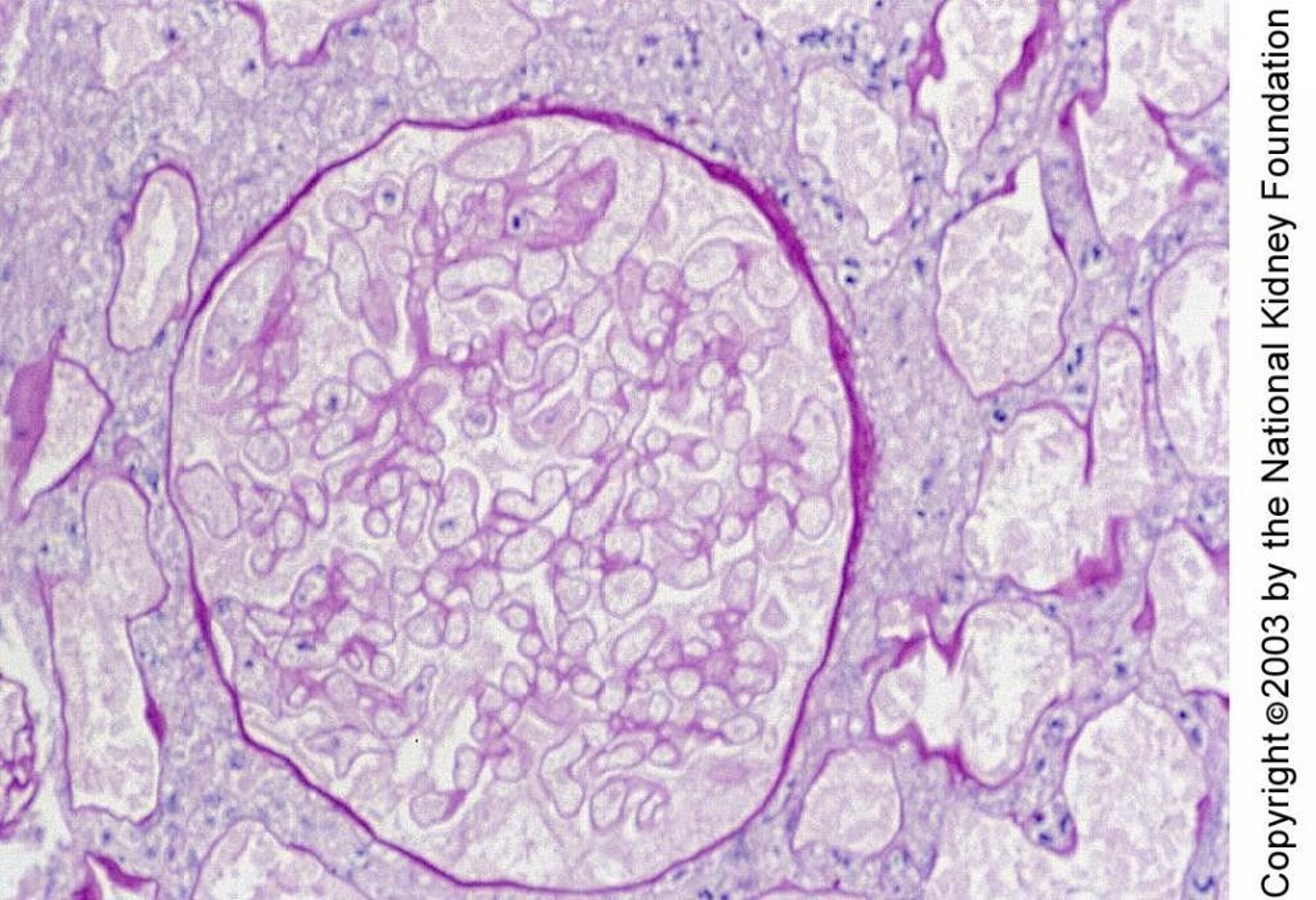
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
If renal or systemic emboli recur and their source is unclear, transesophageal echocardiography is done to detect atheromatous lesions in the ascending and thoracic aorta and cardiac sources of emboli; dual helical CT may help characterize the ascending aorta and aortic arch.
Treatment of Renal Atheroembolism
Treatment of embolic source when possible
Supportive measures
Modification of risk factors
Sometimes the source of emboli can be treated (eg, anticoagulation for patients with emboli from a cardiac source and atrial fibrillation and for patients in whom a clot becomes a source of new emboli). However, no direct treatment of existing renal emboli is effective. Corticosteroids, antiplatelet medications, vasodilators, and plasma exchange are not helpful. There is no demonstrated benefit of anticoagulation and, according to most experts, its use may actually enhance atheroembolism.
Treatment of renal dysfunction includes control of hypertension and management of electrolytes and fluid status; sometimes dialysis is required. Modifying risk factors for atherosclerosis may slow its progression and induce regression. Strategies include management of hypertension, hyperlipidemia, and diabetes; smoking cessation; and encouragement of regular aerobic exercise and good nutrition (Atherosclerosis: Treatment).
Prognosis for Renal Atheroembolism
Patients with renal atheroemboli have a poor overall prognosis.
Key Points
Renal atheroembolism usually results from manipulation of the aorta during vascular surgery, angioplasty, or arteriography, and rarely from spontaneous atherosclerotic embolization.
Suspect the diagnosis if renal function deteriorates after the aorta or another large artery is manipulated.
Confirm the diagnosis based on clinical findings and occasionally with percutaneous renal biopsy.
Treat supportively, correcting modifiable risk factors and, when possible, treating the embolic source; however, the overall prognosis remains poor.






