


(See also Overview of Congenital Cardiovascular Anomalies.)
Patent ductus arteriosus accounts for 5 to 10% of congenital heart anomalies; the male:female ratio is 1:3. PDA is very common among preterm infants (present in about 45% with birth weight < 1750 g and in 70 to 80% with birth weight < 1200 g). About one third of PDAs will close spontaneously, even in extremely low birth weight infants. When persistent in preterm infants, a significant PDA can result in heart failure, exacerbation of lung disease of prematurity, pulmonary hemorrhage, renal insufficiency, feeding intolerance, necrotizing enterocolitis, and even death.
Pathophysiology of PDA
The ductus arteriosus is a normal connection between the pulmonary artery and aorta; it is necessary for proper fetal circulation. At birth, the rise in PaO2 and decline in prostaglandin concentration cause closure of the ductus arteriosus, typically beginning within the first 10 to 15 hours of life. If this normal process does not occur, the ductus arteriosus will remain patent (see figure Patent ductus arteriosus).
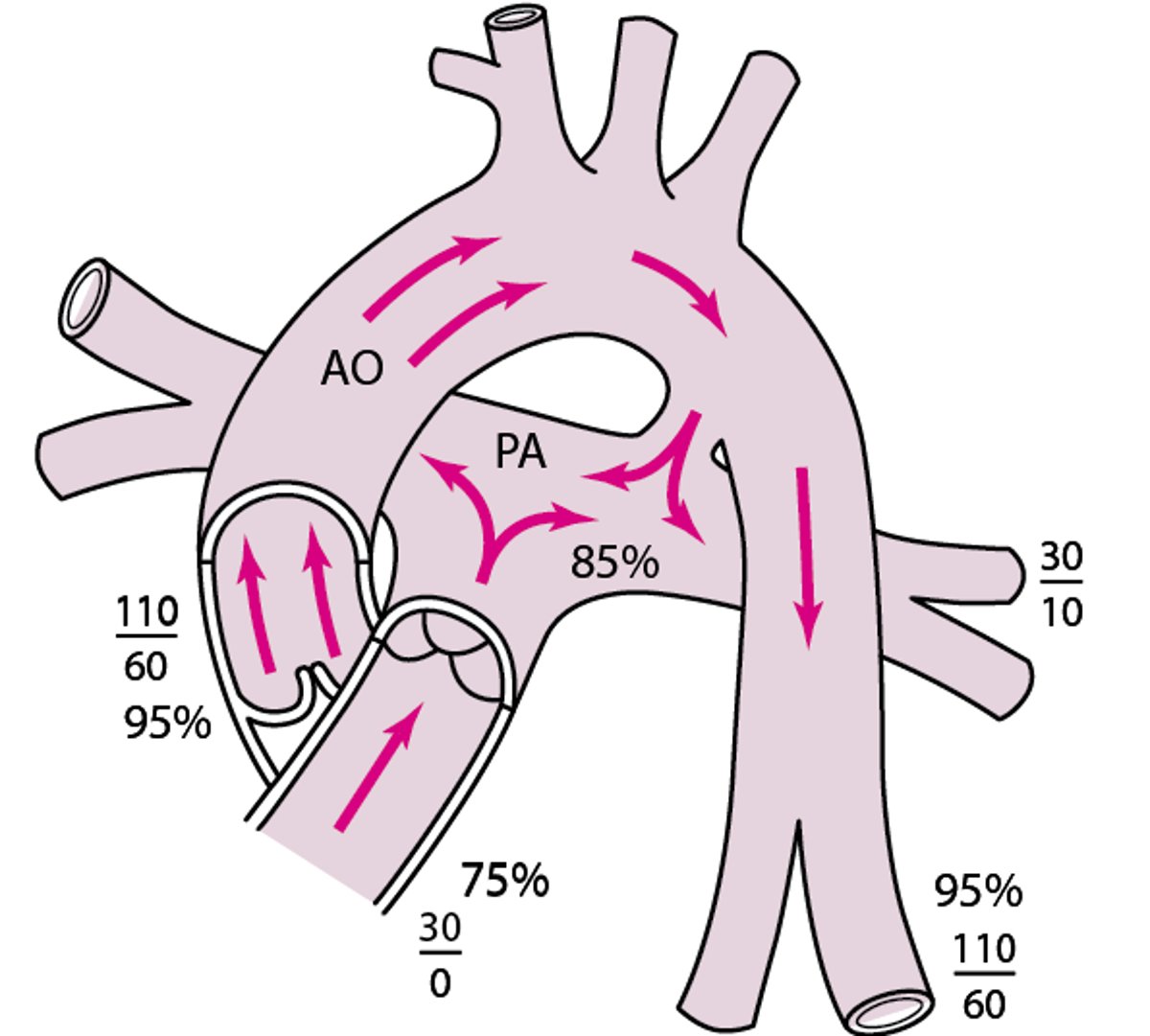
Patent ductus arteriosus
Pulmonary blood flow, LA and LV volumes, and ascending AO volume are increased. AO = aorta; LA = left atrium; LV = left ventricle; PA = pulmonary artery. |

Physiologic consequences depend on ductal size. A small ductus rarely causes symptoms. A large ductus causes a large left-to-right shunt. If uncorrected, over time, a large shunt results in left heart enlargement, pulmonary artery hypertension, and elevated pulmonary vascular resistance, ultimately leading to Eisenmenger syndrome.
Symptoms and Signs of PDA
Clinical presentation depends on patent ductus arteriosus size and gestational age at delivery. Infants and children with a small PDA are generally asymptomatic; infants with a large PDA present with signs of heart failure (eg, failure to thrive, poor feeding, tachypnea, dyspnea with feeding, tachycardia). Preterm infants may present with respiratory distress, apnea, worsening mechanical ventilation requirements, or other serious complications (eg, necrotizing enterocolitis). Signs of heart failure occur earlier in preterm infants than in full-term infants and may be more severe. A large ductal shunt in a preterm infant often is a major contributor to the severity of the lung disease of prematurity.
Most children with a small PDA have normal first and second heart sounds and peripheral pulses. A grade 1 to 3/6 continuous murmur is heard best in the upper left sternal border (see table Heart Murmur Intensity). The murmur extends from systole to beyond the second heart sound (S2) into diastole and typically has a different pitch in systole and diastole.
Full-term infants with a significant PDA shunt have full or bounding peripheral pulses with a wide pulse pressure. A grade 1 to 4/6 continuous murmur is characteristic. If the murmur is loud, it has a “machinery sounding” quality. An apical diastolic rumble (due to high flow across the mitral valve) or gallop rhythm may be audible if there is a large left-to-right shunt or heart failure develops.
Preterm infants with a significant shunt have bounding pulses and a hyperdynamic precordium. A heart murmur occurs in the pulmonary area; the murmur may be continuous, systolic with a short diastolic component, or only systolic, depending on the pulmonary artery pressure. Some infants have no audible heart murmur.
Diagnosis of PDA
Chest x-ray and ECG
Echocardiography
Diagnosis is suggested by clinical examination, supported by chest x-ray and ECG, and established by 2-dimensional echocardiography with color flow and Doppler studies.
Chest x-ray and ECG are typically normal if the patent ductus arteriosus is small. If the shunt is significant, chest x-ray shows prominence of the left atrium, left ventricle, and ascending aorta and increased pulmonary vascular markings; ECG may show left ventricular hypertrophy.
Echocardiography provides important information about the hemodynamic significance of a PDA by assessing a number of parameters, including the
Size of the PDA (often compared to the left pulmonary artery size)
Flow velocity in the PDA
Presence of left heart enlargement
Presence of diastolic reversal of flow in the descending aorta
Presence of diastolic antegrade flow in the left pulmonary artery
Cardiac catheterization is not necessary unless used for therapy.
Treatment of PDA
Supportive medical therapy
Sometimes transcatheter closure or surgical repair
Typical medical management of patent ductus arteriosus includes fluid restriction, a diuretic (usually a thiazide), maintenance of hematocrit ≥ 35 %, providing a neutral thermal environment, and, for ventilated patients, use of positive end-expiratory pressure (PEEP) to improve gas exchange.
Treatment differs depending on whether the infant is preterm or full term.
PDA treatment in preterm infants
Fluid restriction may facilitate ductal closure.
In preterm infants without respiratory or other compromise, a patent ductus arteriosus is typically not treated.
Transcatheter closure of the PDA in the smallest of preterm infants (< 1000 grams) is being done in an increasing number of centers (1).
Indomethacin Dosing Guidelines*
Age at Dose 1 | Dose 1 | Dose 2 | Dose 3 |
|---|---|---|---|
< 48 hours | 0.2 mg/kg IV | 0.1 mg/kg IV | 0.1 mg/kg IV |
2–7 days | 0.2 mg/kg IV | 0.2 mg/kg IV | 0.2 mg/kg IV |
> 7 days | 0.2 mg/kg IV | 0.25 mg/kg IV | 0.25 mg/kg IV |
* Dose intervals are based on urine output (see text). | |||
PDA treatment in full-term infants
In full-term infants, COX inhibitors are usually ineffective.
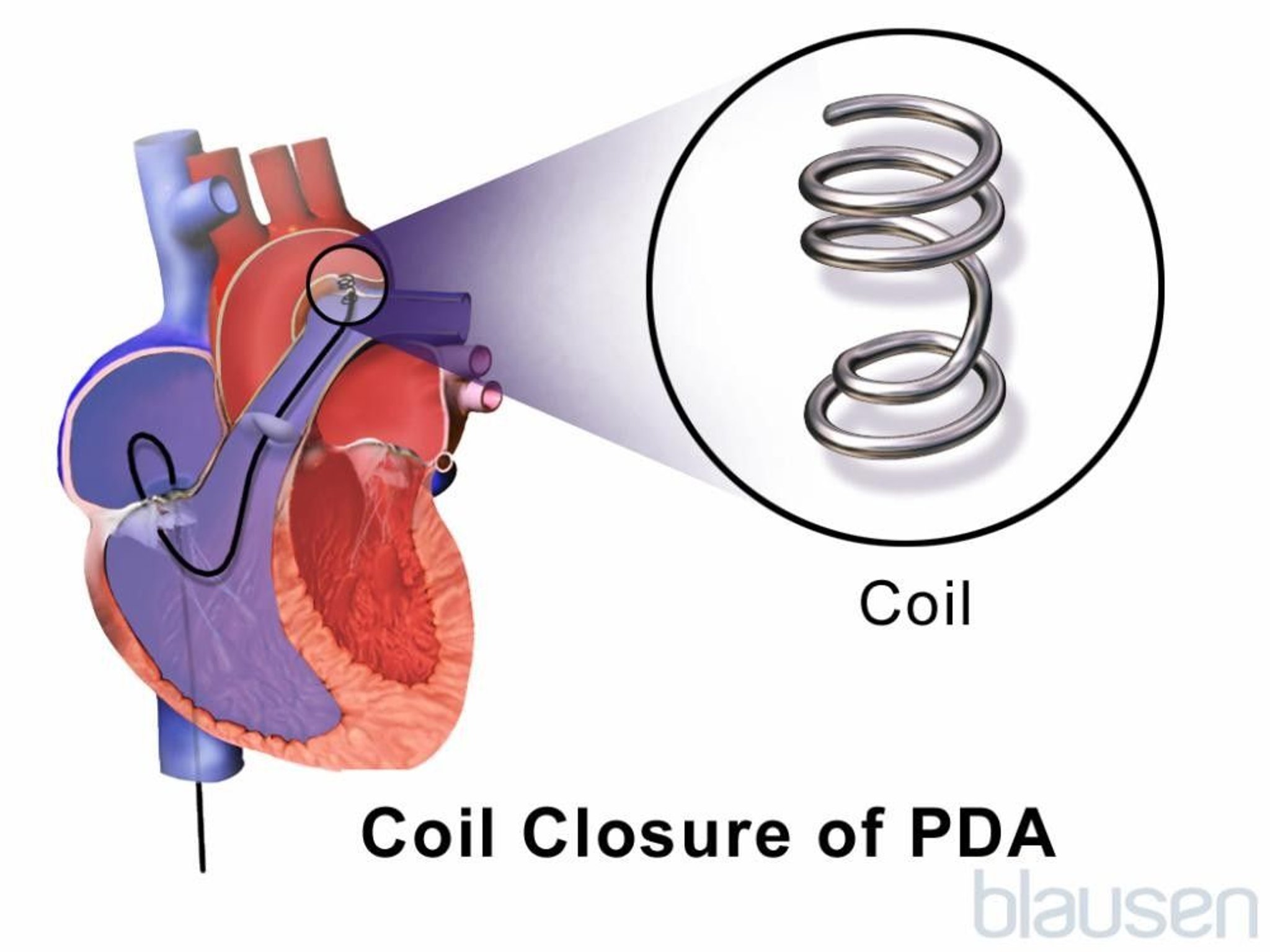
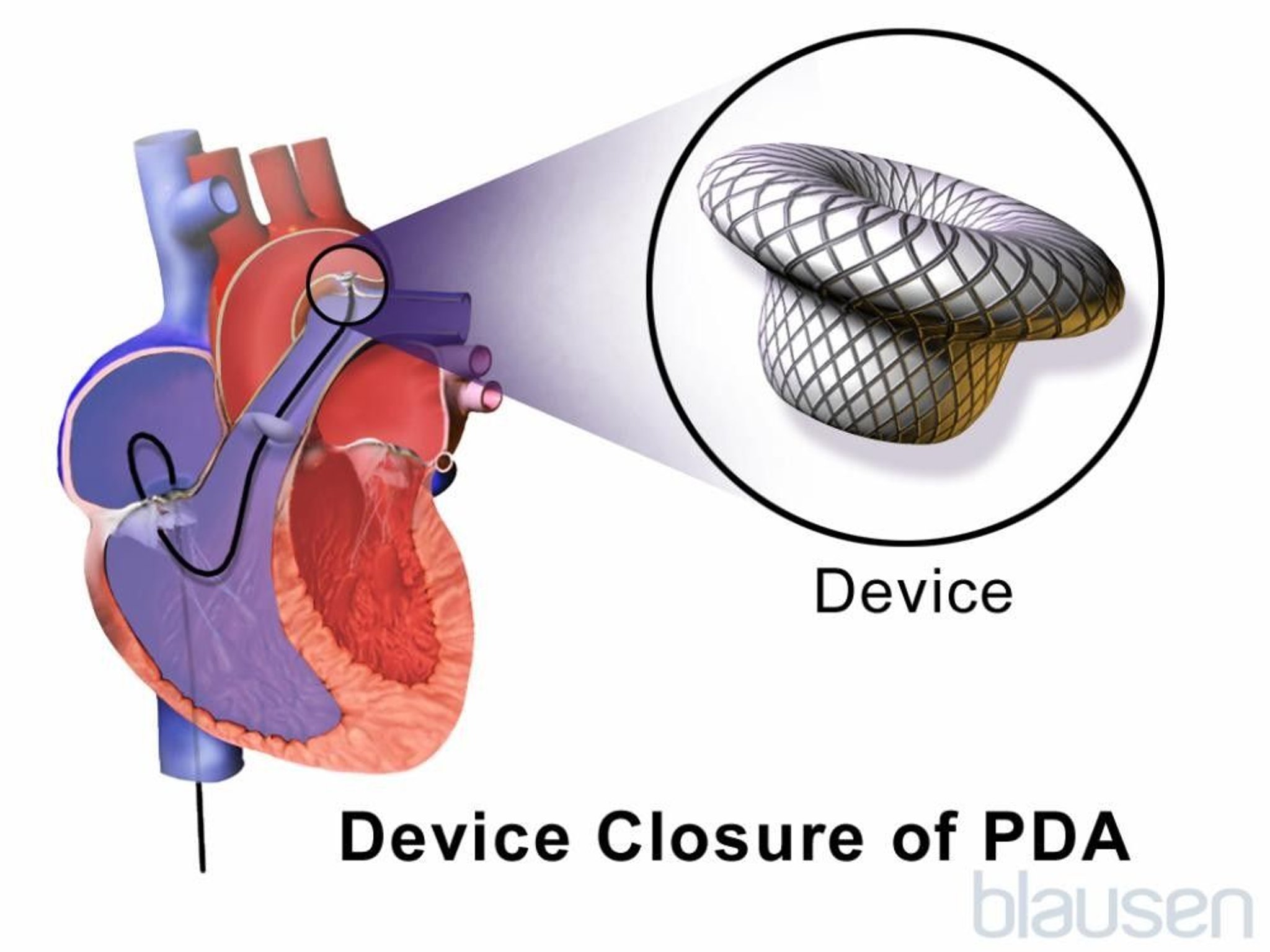
Transcatheter closure has become the treatment of choice for PDA in children > 1 year, and some authors consider transcatheter closure to be the preferred route in term neonates and young infants as well. A variety of catheter-delivered occlusion devices are available (eg, coils, septal duct occluder).
In infants < 1 year who have ductal anatomy unfavorable for transcatheter closure, surgical division and ligation may be preferred over the transcatheter approach. For a patent ductus arteriosus with a shunt large enough to cause symptoms of heart failure or pulmonary hypertension, closure should be done after medical stabilization. For a persistent PDA without heart failure or pulmonary hypertension, closure can be done electively any time after 1 year. Delaying the procedure minimizes the risk of a vascular complication and allows time for spontaneous closure.
Outcomes after PDA closure are excellent.

Endocarditis prophylaxis is not needed preoperatively and is required only for the first 6 months after closure or if there is a residual defect adjacent to a transcatheter-placed device or surgical material.
Treatment reference
1. Philip R, Tailor N, Johnson JN, et al: Single-Center Experience of 100 Consecutive Percutaneous Patent Ductus Arteriosus Closures in Infants ≤1000 Grams. Circ Cardiovasc Interv 14(6):e010600, 2021. doi:10.1161/CIRCINTERVENTIONS.121.010600
Key Points
Patent ductus arteriosus (PDA) is a persistence after birth of the normal fetal connection (ductus arteriosus) between the aorta and pulmonary artery, resulting in a left-to-right shunt.
Manifestations depend on the size of the PDA and the age of the child, but a continuous murmur is characteristic and, if loud, has a “machinery sounding” quality.
Preterm infants may have respiratory distress or other serious complications (eg, necrotizing enterocolitis).
Over time, a large shunt causes left heart enlargement, pulmonary artery hypertension, and elevated pulmonary vascular resistance, ultimately leading to Eisenmenger syndrome if untreated.
For full-term infants and older children, COX inhibitors are usually ineffective, but a catheter-delivered occlusion device or surgery typically provides long-term correction of this anomaly.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers






