


View Patient Education
The most common testicular and scrotal anomalies are
Congenital hydrocele
Undescended testes (cryptorchidism)
Rare anomalies include scrotal agenesis, hypoplasia, ectopia, or hemangioma; penoscrotal transposition; and bifid scrotum.
Congenital hydrocele
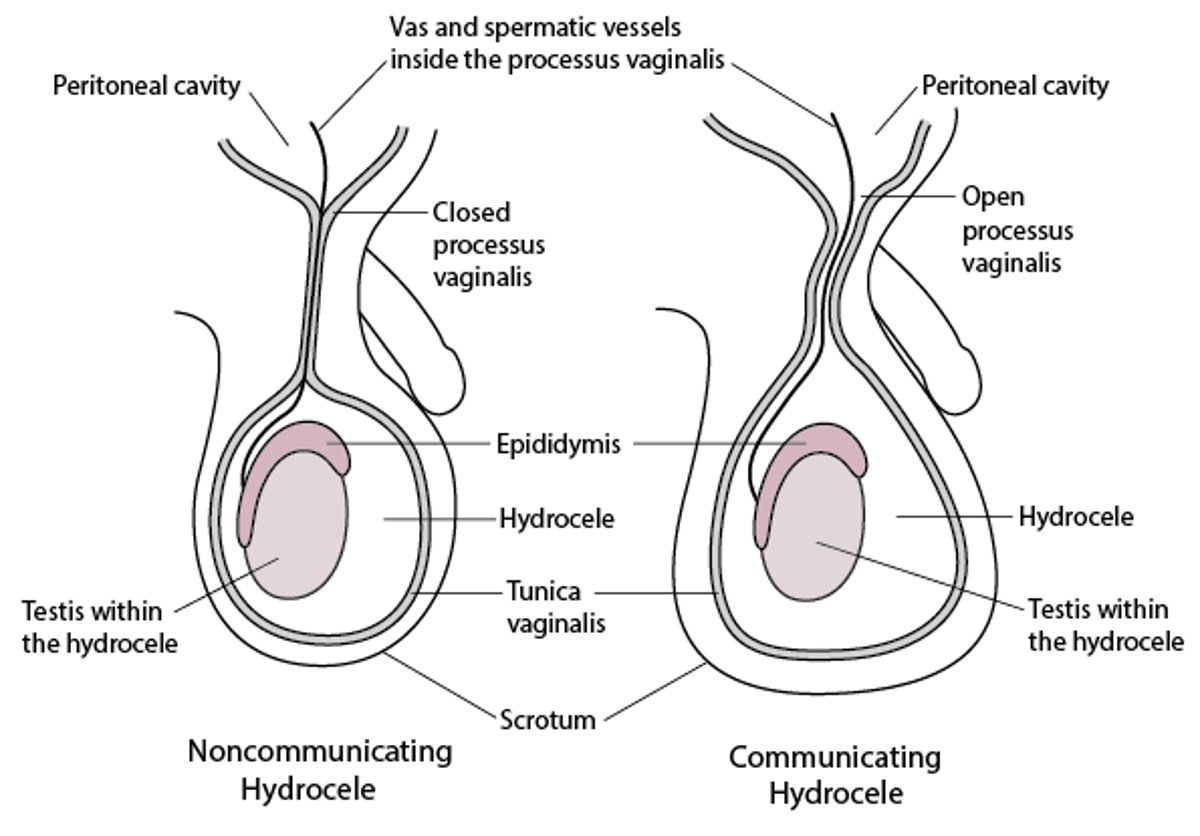
A congenital hydrocele is a collection of fluid in the scrotum between layers of the tunica vaginalis. It may be isolated (noncommunicating) or may communicate with the abdominal cavity through a patent processus vaginalis (a potential hernia space). Hydrocele manifests as a painless, enlarged scrotum. The condition may resolve spontaneously but usually requires repair if it persists after 12 months or if it enlarges.
Congenital hydrocele

Congenital Hydrocele


Hide Details
This photo shows marked scrotal swelling caused by a hydrocele. Note the absence of inflammation.
© Springer Science+Business Media


Test your KnowledgeTake a Quiz!




