


Sprains of the external (medial and lateral collateral) or internal (anterior and posterior cruciate) ligaments or injuries of the menisci may result from knee trauma. Symptoms include pain, joint effusion, instability (with severe sprains), and locking (with some meniscal injuries). Diagnosis is by physical examination and sometimes MRI. Treatment is PRICE (protection, rest, ice, compression, elevation) and, for severe injuries, casting or surgical repair.
(See also Overview of Sprains and Other Soft-Tissue Injuries.)
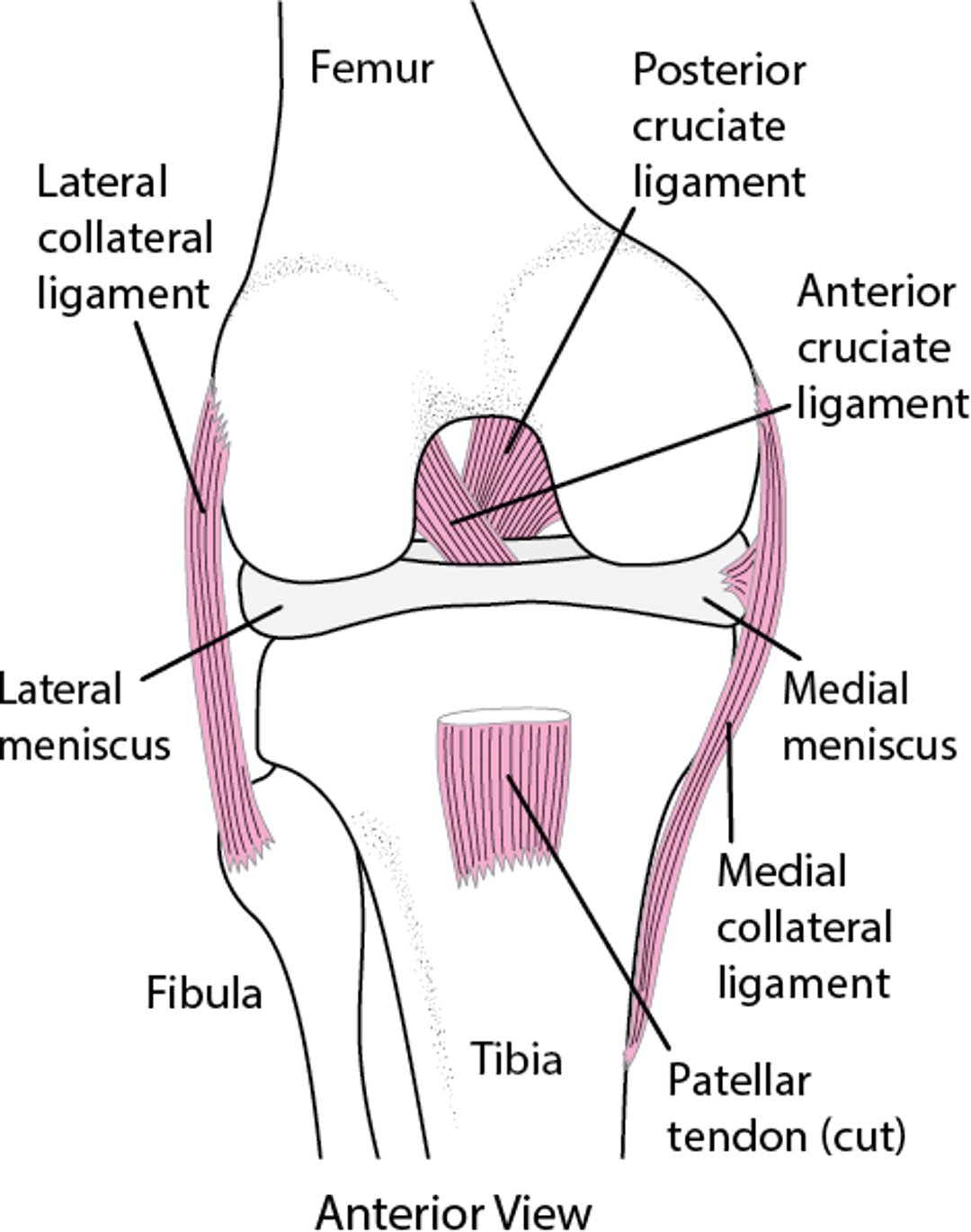
Many structures that help stabilize the knee are located mainly outside the joint; they include muscles (eg, quadriceps, hamstrings), their insertions (eg, pes anserinus), and extracapsular ligaments. The lateral collateral ligament is extracapsular; the medial (tibial) collateral ligament has a superficial extracapsular portion and a deep portion that is part of the joint capsule.
Inside the knee, the joint capsule and the posterior and highly vascular anterior cruciate ligaments help stabilize the joint. The medial and lateral menisci are intra-articular cartilaginous structures that act mainly as shock absorbers but provide some stabilization (see figure Ligaments of the knee).
Ligaments of the knee

The most commonly injured knee structures are the
Medial collateral ligament
Anterior cruciate ligament
The mechanism of injury predicts the type of injury:
Inward (valgus) force: Usually, the medial collateral ligament, followed by the anterior cruciate ligament, then the medial meniscus (this mechanism is the most common and is usually accompanied by some external rotation and flexion, as when being tackled in football)
Outward (varus) force: Often, the lateral collateral ligament, anterior cruciate ligament, or both (this mechanism is the 2nd most common)
Anterior or posterior forces and hyperextension: Typically, the cruciate ligaments
Weight bearing and rotation at the time of injury: Usually, menisci

Symptoms and Signs of Knee Sprains and Meniscal Injuries
Swelling and muscle spasm progress over the first few hours. With 2nd-degree sprains, pain is typically moderate or severe. With 3rd-degree sprains, pain may be mild, and surprisingly, some patients can walk unaided.
Some patients hear or feel a pop when the injury occurs. This finding suggests an anterior cruciate ligament tear but is not a reliable indicator.
Location of the tenderness and pain depends on the injury:
Sprained medial or lateral ligaments: Tenderness over the damaged ligament
Medial meniscal injuries: Tenderness in the joint plane (joint line tenderness) medially
Lateral meniscal injuries: Tenderness in the joint plane laterally
Medial and lateral meniscal injuries: Pain made worse by extreme flexion or extension and restricted passive knee motion (locking)
Injuries of any of the knee ligaments or menisci cause a visible and palpable joint effusion.
The ballottement (patellar tap) test can be used to check for joint effusion. It is best done when the patient lies supine. The examiner uses one hand to firmly slide down the quadriceps muscles toward the knee and stops several centimeters above the knee joint. With the other hand, the examiner taps on the patella. If the patella bounces (ballottes), the patella is floating in fluid, indicating a significant knee joint effusion.
Diagnosis of Knee Sprains and Meniscal Injuries
Clinical evaluation
X-rays to exclude fractures
Sometimes MRI
Diagnosis of knee sprains and meniscal injuries is primarily clinical. Stress testing is usually delayed because the pain is so great initially.
A spontaneously reduced knee dislocation should be suspected in patients with a large hemarthrosis, gross instability, or both; detailed vascular evaluation, including ankle-brachial index (ABI), and CT angiography should be done immediately because popliteal artery injury is possible. Next, the knee is fully examined. Active knee extension is assessed in all patients with knee pain and effusion to check for disruption of the knee extensor mechanism (eg, tears of the quadriceps or patellar tendon, fracture of the patella or tibial tubercle).
Pearls & Pitfalls
|
Stress testing
Stress testing to evaluate ligament integrity helps distinguish partial from complete tears. However, if patients have significant pain and swelling or muscle spasm, testing is typically delayed until x-rays exclude fractures. Also, significant swelling and spasm may make joint stability difficult to evaluate. Such patients should be examined 2 to 3 days later (after swelling and spasm have subsided). A delayed physical examination of the knee is more sensitive than MRI of the knee (86% vs 76% [1]) for diagnosis of meniscal and anterior cruciate ligament injuries.
Bedside stress testing is done to check for specific injuries, although most of these tests are not highly accurate or reliable. For bedside stress testing, clinicians move the joint in a direction in which the ligament being tested normally prevents excessive joint movement.
For the Apley test, the patient is prone, and the examiner stabilizes the patient’s thigh. The examiner flexes the patient’s knee 90° and rotates the lower leg while pressing the lower leg downward toward the knee (compression), then rotates the lower leg while pulling it away from the knee (distraction). Pain during compression and rotation suggests a meniscal injury; pain during distraction and rotation suggests a ligamentous or joint capsule injury.
For evaluation of the medial and lateral collateral ligaments, the patient is supine, with the knee flexed about 20° and the hamstring muscles relaxed. The examiner puts one hand over the side of the knee opposite the ligament being tested. With the other hand, the examiner cups the heel and pulls the lower leg outward to test the medial collateral ligament or inward to test the lateral collateral ligament. Moderate instability after acute injury suggests that a meniscus or cruciate ligament is torn as well as the collateral ligament.
The Lachman test is the most sensitive physical test for acute anterior cruciate ligament tears (2). With the patient supine, the examiner supports the patient’s thigh and calf, and the patient’s knee is flexed 20°. The lower leg is moved anteriorly. Excessive passive anterior motion of the lower leg from the femur suggests a significant tear.
Imaging
Not every patient requires x-rays. However, anteroposterior, lateral, and oblique x-rays are often taken to exclude fractures. The Ottawa knee rules are used to limit x-rays to patients more likely to have a fracture that requires specific treatments. X-rays should be taken only if one of the following is present:
Age > 55
Isolated tenderness of the patella (with no other bone tenderness of the knee)
Tenderness of fibular head
Inability to flex the knee 90°
Inability to bear weight both immediately and in the emergency department for 4 steps (with or without limping)
MRI is usually not needed at the initial evaluation. A reasonable approach is to do MRI if symptoms do not resolve after a few weeks of conservative management. However, MRI is often done when severe injury or significant intra-articular injury is suspected or cannot be otherwise excluded.
Other tests may be done to check for related injuries:
Arteriography or CT angiography to check for suspected arterial injuries if knee dislocation or severe hyperextension are suspected
Electromyography and/or nerve conduction studies, which are rarely done immediately but more typically done when nerve symptoms persist weeks to months after the injury
Diagnosis references
1. Rayan F, Bhonsle S, Shukla DD: Clinical, MRI, and arthroscopic correlation in meniscal and anterior cruciate ligament injuries. Int Orthop 2009 33 (1):129–132, 2009. doi: 10.1007/s00264-008-0520-4
2. Benjaminse A, Gokeler A, van der Schans CP: Clinical diagnosis of an anterior cruciate ligament rupture: A meta-analysis. J Orthop Sports Phys Ther 36 (5):267–288, 2006. doi:10.2519/jospt.2006.2011
Treatment of Knee Sprains and Meniscal Injuries
Mild sprains: Protection, rest, ice, compression, and elevation (PRICE) with early mobilization
Severe injuries: Splinting or a knee immobilizer and referral to an orthopedic surgeon for surgical repair
Draining large effusions (see figure Arthrocentesis of the knee) may decrease pain and spasm. Contraindications to knee arthrocentesis include anticoagulation and cellulitis overlying the affected knee.
Most 1st-degree and moderate 2nd-degree injuries can be treated initially with PRICE. Early range of motion exercises are usually encouraged. Knee immobilizers are rarely recommended for sprains and strains.
Severe 2nd-degree and most 3rd-degree sprains require casting for ≥ 6 weeks.
Some 3rd-degree injuries of the medial collateral ligament and anterior cruciate ligament require arthroscopic surgical repair. Patients with severe injuries are referred to an orthopedic surgeon for surgical repair.
Meniscal injuries vary widely in their characteristics and treatments. Large, complex, or vertical tears and injuries that result in persistent effusions or disabling symptoms are more likely to require surgery. Patient preference can influence choice of treatment.
Physical therapy may be helpful, depending on the patient and the type of injury.
Early mobilization is NOT recommended for minor sprains. Immobilizers should be used only by patients with an unstable knee or a fracture and only until they are seen by an orthopedic surgeon. The optimal immobilization duration is unclear (1).
Treatment reference
1. Sommerfeldt M, Bouliane M, Otto D, et al: The use of early immobilization in the management of acute soft-tissue injuries of the knee: results of a survey of emergency physicians, sports medicine physicians and orthopedic surgeons. Can J Surg 58(1):48-53, 2015. doi:10.1503/cjs.004014
Key Points
Stress testing (usually done days after the injury) is necessary for differentiation of partial from complete ligamentous tears and is more sensitive than MRI.
Consider injury to the anterior cruciate ligament and other intra-articular structures if patients have an effusion after an injury.
Consider knee dislocation and popliteal artery injury if patients have a large hemarthrosis, gross instability, or both.
If patients have knee pain and effusion, test active knee extension to check for disruption of the extensor mechanism (eg, tears of the quadriceps or patellar tendon, fracture of the patella or tibial tubercle).
Do MRI if symptoms do not resolve after a few weeks of conservative management or possibly when severe injury or significant intra-articular injury is suspected or cannot be otherwise excluded.






