


View Patient Education
Pharmacogenetics involves variations in drug response due to genetic makeup.
The activity of drug-metabolizing enzymes often varies widely among healthy people, making metabolism highly variable. Drug elimination rates vary up to 40-fold. Genetic factors and aging seem to account for most of these variations.
Pharmacogenetic variation (eg, in acetylation, hydrolysis, oxidation, or drug-metabolizing enzymes) can have clinical consequences (see table Examples of Pharmacogenetic VariationsGenetic, environmental, and developmental factors that can interact).
Table
Examples of Pharmacogenetic Variations
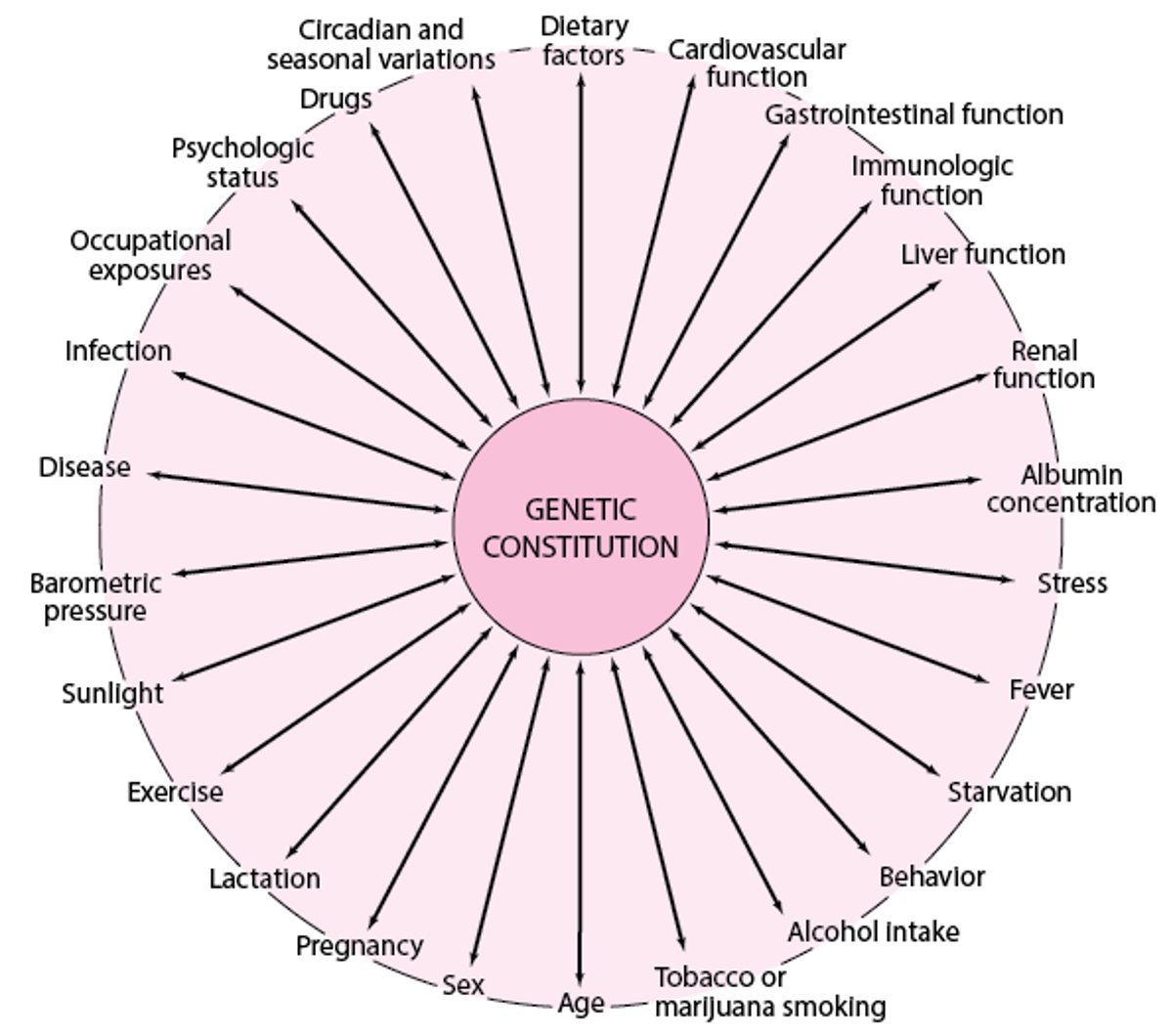
Genetic, environmental, and developmental factors that can interact, causing variations in drug response among patients

Drugs Mentioned In This Article


Test your KnowledgeTake a Quiz!




