


Ocular burns can occur after thermal or chemical injuries and can result in serious complications, including permanent blindness.
(See also Overview of Eye Trauma.)
Thermal burns
Chemical burns
Chemical burns of the cornea and conjunctiva represent 11 to 22% of ocular trauma and can be serious, particularly when strong acid or alkali is involved. Alkali burns cause liquefaction necrosis, whereas acid burns cause coagulation necrosis. Because of this difference, alkali burns have deeper penetration and tend to be more serious than acid burns.

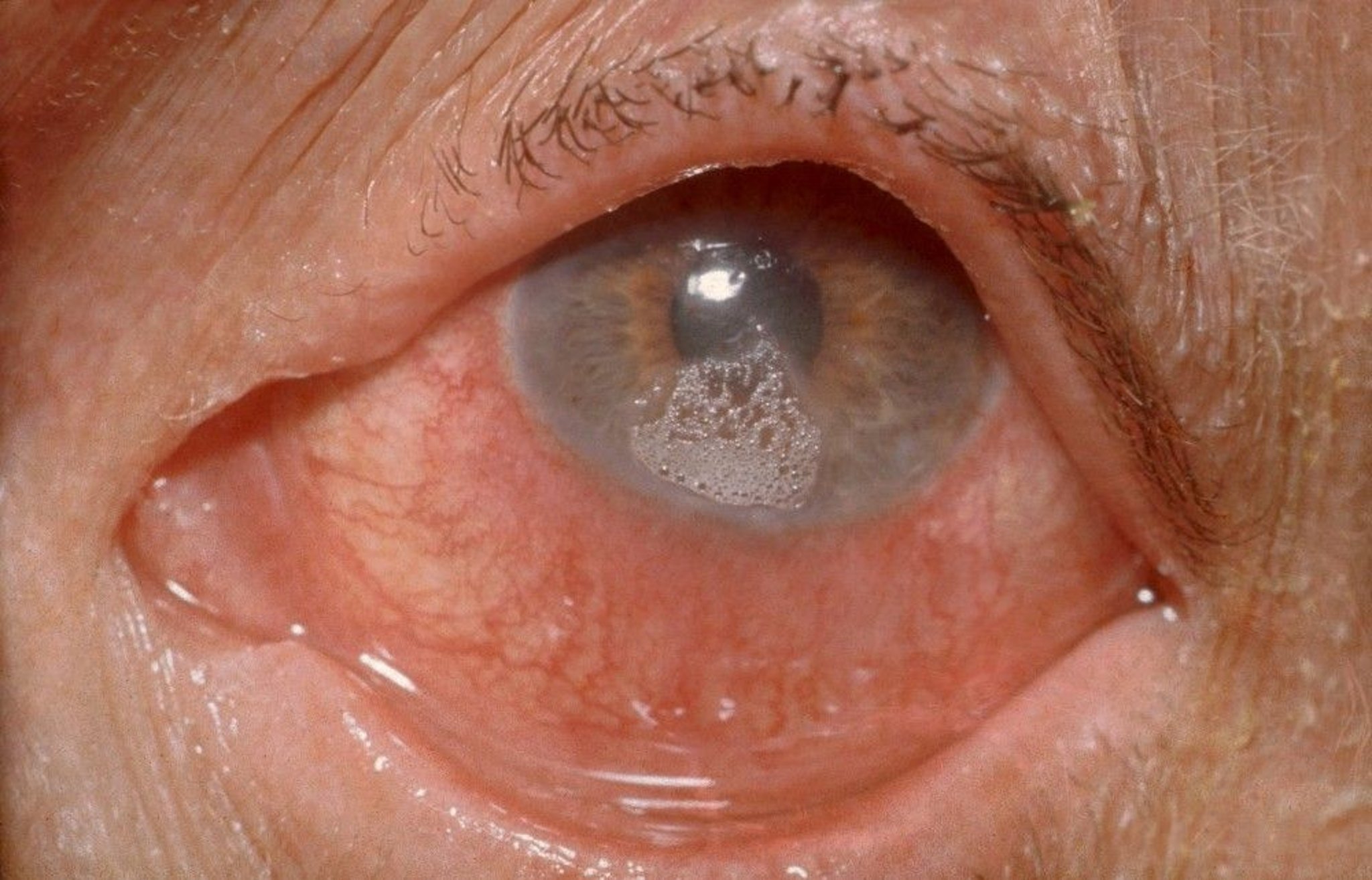
Clinical Photography/SCIENCE PHOTO LIBRARY
Pearls & Pitfalls
|
After irrigation, the conjunctival fornices should be examined for chemical embedded in the tissue and swept with a swab to remove trapped particles. The superior fornices are exposed by using double eyelid eversion (ie, first everting the eyelid and then inserting a swab under the everted eyelid and lifting it up until the fornix is visible).
Mild chemical burns
Severe chemical burns
Chemical iritis is suspected in patients with photophobia (deep eye pain with exposure to light) that develops hours or days after a chemical burn and is diagnosed by finding flare and white blood cells in the anterior chamber during slit-lamp examination
Key Points
Thermal burns tend to affect the eyelid, whereas chemical burns can affect the eyelid, conjunctiva, and cornea.
Treat thermal burns with topical antimicrobials, cycloplegic mydriatics (if conjunctiva or cornea are affected), and oral analgesics.
Rapid and copious irrigation is vital after a chemical burn; a borate buffer solution or balanced saline solution are best but any sterile saline solution or water can be used.
Prescribe topical antibiotics and cycloplegic mydriatics after irrigation of a chemical burn.
For moderate or severe burns, consult an ophthalmologist for consideration of further therapy.
More Information
The following are some English-language resources that may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Sharma N, Kaur M, Agarwal T, et al: Treatment of acute ocular chemical burns. Surv Ophthalmol 63(2):214-235, 2018. doi:10.1016/j.survophthal.2017.09.005
Baradaran-Rafii A, Eslani M, Haq Z, Shirzadeh E, et al: Current and upcoming therapies for ocular surface chemical injuries. Ocul Surf 15(1):48-64, 2017. doi:10.1016/j.jtos.2016.09.002






